
Introduction to the Commonwealth Coordinated Care Program
The Commonwealth Coordinated Care (CCC) program represents a significant initiative in Virginia, designed to streamline and enhance the delivery of crucial healthcare services. This innovative program focuses on individuals who are dually eligible for both Medicaid and Medicare, often referred to as “dual eligibles.” By integrating primary, preventive, acute, behavioral, and long-term services and supports, the CCC program aims to create a more coordinated and efficient healthcare experience for this vulnerable population.
Virginia stands as one of twelve states collaborating with the Centers for Medicare and Medicaid Services (CMS) in a pioneering effort known as the Financial and Administrative Alignment Demonstration for Dual Eligible Beneficiaries. The CCC program is a flagship example of this collaboration, being among the first to be implemented. Launched in March 2014, with beneficiary enrollment commencing in April of the same year, this program was initially set to run until December 31, 2017.
| Box 1: The Duals Demos: Financial and Administrative Alignment Demonstrations |
|---|
| Empowered by the Affordable Care Act, CMS is rigorously testing capitated and managed fee-for-service models to financially align and enhance care coordination for dual-eligible beneficiaries. These demonstrations are driven by the dual goals of improving healthcare outcomes and controlling costs for a demographic comprising both seniors and non-elderly individuals with significant disabilities. These three-year demonstrations, initiated in July 2013, are fundamentally reshaping care delivery systems for beneficiaries receiving medical and long-term care. They are also transforming the financial relationships between CMS, state governments, and healthcare providers. As of February 2015, CMS had finalized Memoranda of Understanding (MOUs) with 11 states to implement these demonstrations. States like California, Illinois, Massachusetts, Michigan, New York, Ohio, South Carolina, Texas, and Virginia are piloting a capitated financial alignment model. Meanwhile, Colorado and Washington are testing a managed fee-for-service (FFS) financial alignment model. Minnesota is exploring administrative function integration without financial alignment. By February 2015, nine states had already started enrolling beneficiaries in their respective programs. For more detailed information, refer to the Kaiser Commission on Medicaid and the Uninsured report, “State Demonstration Proposals to Integrate Care and Align Financing and/or Administration for Dual Eligible Beneficiaries” (February 2015), accessible at: https://www.kff.org/medicaid/fact-sheet/state-demonstration-proposals-to-integrate-care-and-align-financing-for-dual-eligible-beneficiaries/ |
Initially, approximately 78,600 Virginians were identified as eligible for the CCC program, which operates across five designated regions within the state. 1 The program’s implementation was carefully phased, offering eligible individuals the choice to enroll or opt-out. Enrollees could select or were assigned to one of three participating managed care plans, known as Medicaid-Medicare Plans (MMPs). These MMPs were entrusted with the responsibility of overseeing and coordinating a more comprehensive suite of healthcare services.
Before the introduction of the CCC program, Medicare beneficiaries in Virginia who were dually eligible rarely enrolled in Medicare Advantage plans. While Virginia had experience delivering Medicaid services through managed care plans, dual-eligible beneficiaries were excluded from these arrangements. Consequently, many healthcare providers serving this population had limited exposure to managed care models. This demonstration also marked a significant shift in Virginia’s approach to providing long-term services and supports (LTSS). Prior to this initiative, a broadly accessible managed LTSS option was not available in Virginia. 2
This analysis delves into the early experiences of dual-eligible beneficiaries and various stakeholders involved in Virginia’s CCC program. It outlines the program’s essential features, highlights its initial successes, and discusses the strategies employed to overcome early challenges. This case study draws upon interviews conducted with state officials, service providers, plan administrators, advocates, and other key stakeholders. These interviews were primarily conducted during an on-site visit to Richmond, Virginia, in late October 2014, supplemented by phone interviews between July and November of the same year. The findings presented here reflect insights gathered from nearly 50 individuals, including state officials, representatives from provider organizations, participating health plans, and consumer advocacy groups, all of whom openly discussed their experiences with the program. Additional information was gleaned from publicly available materials on the program website and data provided by program officials.
As an early evaluation of Virginia’s CCC program, this case study aims to provide valuable insights into the initial hurdles and solutions encountered. This information is intended to be beneficial for other states embarking on similar program implementations. However, it’s crucial to recognize that while this study emphasizes early challenges, it also addresses broader program design and policy considerations that are vital for the program’s long-term success and sustainability. These wider issues were also explored and are reported in this analysis.
Program Features of the Commonwealth Coordinated Care Program
Program Administration
The Department of Medical Assistance Services (DMAS), Virginia’s state Medicaid agency, is the primary administrative body for the Commonwealth Coordinated Care Program. The Department of Aging and Rehabilitative Services (DARS) also plays a crucial supporting role. Program staff have earned a strong reputation among stakeholders for their dedication and commitment to the program’s success. Many individuals within these departments have long been involved in initiatives aimed at improving service delivery for Medicaid medical and long-term services and supports. Despite this experience, one official described the CCC program rollout as “more challenging than anything DMAS has ever undertaken,” emphasizing the critical role of broad political support throughout the program’s development and implementation. Notably, the demonstration proposal gained bipartisan support, originating during the administration of Republican Governor Bob McDonnell and being implemented under Democratic Governor Terry McAuliffe.
Unlike some other demonstration states, Virginia did not receive an early federal design contract for program development. However, the state has made substantial investments, creating new positions, recruiting staff, applying for relevant federal grants, implementing significant data system upgrades, conducting extensive stakeholder education and communication, and funding an early state-specific program evaluation. CMS serves as a vital partner in this demonstration project.
Outreach and Enrollment Strategies
At the program’s inception, an estimated 78,600 dual-eligible beneficiaries across five regions of Virginia were deemed eligible for CCC program participation. 3 Approximately one-third of this group was already receiving long-term services and supports, with 17 percent residing in nursing facilities and 13 percent participating in the Elderly or Disabled with Consumer Direction (EDCD) waiver program. 4 The remaining 70 percent lived in the community and were not enrolled in a waiver program. 5
Enrollment Information and Support: To facilitate enrollment and address beneficiary inquiries, the state contracted with an enrollment broker, compensating them with a flat fee for each enrollment assistance provided. This broker assists beneficiaries with enrollment procedures and answers questions regarding MMP characteristics, such as provider networks, drug formularies, and enhanced benefits. The CCC program also collaborates closely with the Virginia Insurance Counseling and Assistance Program (VICAP), a federally funded state health insurance assistance program. VICAP offers personalized counseling and support, primarily through volunteers, to Medicare beneficiaries and their families, either in person or via telephone. 6 To enhance VICAP’s capacity to support the CCC program, a federal grant enabled the hiring of an Options Counseling Coordinator. This coordinator manages beneficiary inquiries about the CCC program and conducts outreach events across the state for both beneficiaries and providers, including sessions at nursing facilities and senior housing complexes. This new role has significantly bolstered the state office’s ability to handle CCC-related inquiries from beneficiaries and local VICAP counselors. While DMAS anticipated VICAP counselors playing a pivotal role in explaining the CCC program, some counselors expressed feeling inadequately informed about specific program details. Consequently, they often directed clients to the enrollment broker for more detailed assistance. Additionally, VICAP agencies faced limitations in providing counseling services in languages other than English.
DMAS further demonstrated its commitment to outreach by hiring a dedicated outreach specialist for the CCC program and hosting regular informational calls for beneficiaries and their advocates. Despite these extensive efforts, stakeholder feedback indicated ongoing questions about beneficiaries’ comprehensive understanding of the new program. Some counselors were impressed by the informed questions from beneficiaries, while others noted a “broad awareness of change, but not so much on the specifics,” or observed a “tremendous amount of confusion.” It was also noted that obtaining complete information often required beneficiaries to navigate multiple sources, such as contacting VICAP and then directly contacting plans for up-to-date provider network information.
Several challenges were identified as contributing to the perceived lack of beneficiary awareness:
- Program and plan staff reported difficulties in reaching eligible beneficiaries, particularly when accurate contact information was unavailable. This made it challenging to confirm if beneficiaries who did not respond to program communications had actually received them.
- Respondents highlighted that some beneficiaries had limited health insurance literacy, potentially hindering their understanding of managed care concepts. For instance, beneficiaries might not fully grasp that a managed care plan’s provider network could offer fewer choices compared to a fee-for-service model. They might also not realize that their current healthcare providers might not participate in the new program.
- Concerns were raised about certain beneficiaries’ capacity to make informed coverage decisions, especially those with cognitive impairments without designated legal representatives to assist them.
- Respondents generally observed a limited focus on reaching “hard to reach” populations. Resources, counseling, and awareness initiatives appeared to be insufficient for populations whose primary language was not English or whose cultural background differed significantly from the mainstream. While introductory letters were available in multiple languages and the enrollment broker offered translation services, targeted outreach efforts remained limited at the time of this study.
The Enrollment Process: The CCC program’s enrollment process was designed to provide multiple opportunities for beneficiaries to opt in or out and to select from the three available MMPs: Anthem HealthKeepers, Humana Gold Plus Integrated, and Virginia Premier Complete Care. Each eligible individual received up to four informational letters. The initial letter introduced the program and offered the opportunity to voluntarily select an MMP. This letter also clearly stated the beneficiary’s right to opt out of the program. Approximately three months after the initial letter, beneficiaries who had neither chosen a plan nor opted out received a subsequent letter. This letter informed them that they would be automatically enrolled in an MMP within 60 days unless they proactively selected a plan or opted out. A follow-up letter, sent 30 days later, reiterated this information. 7 Following enrollment, whether voluntary or automatic, health plans sent welcome packages to all new enrollees. Beneficiaries were continuously informed of their ongoing ability to opt in, opt out, or switch plans at any time.
The enrollment process was rolled out in phases across the five regions throughout 2014. This phased approach allowed program administrators to refine operational processes in later regions based on lessons learned from earlier implementations. Coverage for the first group of voluntary enrollees in the Tidewater and Central Virginia regions commenced on April 1, 2014. The first round of automatic enrollment in these regions followed on July 1, 2014, and September 1, 2014, respectively. 8 Shortly after the outreach and enrollment process began in the initial two regions, the same process was initiated in the remaining three regions (as detailed in Table 1).
| Table 1: 2014 Enrollment Schedule for Virginia’s CCC Program |
|---|
| Region |
| Tidewater |
| Central Virginia |
| Charlottesville |
| Roanoke |
| Northern Virginia |
| SOURCE: Commonwealth Coordinated Care Enrollment Timeline and Update, July 2014. Available at: http://www.dmas.virginia.gov/content_pgs/altc-stkhld.aspx. |
Plan Assignment Strategy: A notable feature of the CCC program was the implementation of an “intelligent assignment” process for automatic enrollment. This process aimed to prioritize continuity of care by considering beneficiaries’ existing healthcare provider relationships when assigning them to MMPs. 9 The objective was to assign beneficiaries to MMPs whose provider networks included their current primary care physicians, specialists, and hospitals, whenever possible. Ideally, plan assignments would be based on Medicare and Medicaid claims data, providing insights into beneficiaries’ healthcare utilization patterns. However, as one of the earliest demonstrations, Virginia faced a challenge as anticipated Medicare data was not readily available at the program’s outset. Consequently, initial assignments relied on alternative data sources, such as previous health plan enrollment for beneficiaries in Medicare Advantage plans and plan network participation by the beneficiary’s nursing facility or adult day health provider. 10
Despite the intelligent assignment approach, respondents reported instances where beneficiaries were assigned to plans whose networks did not include their established providers. Even when assignments were based on nursing facility residence, the physicians caring for patients within those facilities were sometimes not included in MMP networks. The state anticipated that access to Medicare data from CMS in future automatic enrollments would improve the accuracy of assignments. Stakeholders also pointed out that even with primary care provider data, optimal matching might be challenging as beneficiaries often have strong relationships with specialists like cardiologists or endocrinologists, or with personal care providers. They suggested considering these relationships in future assignment refinements.
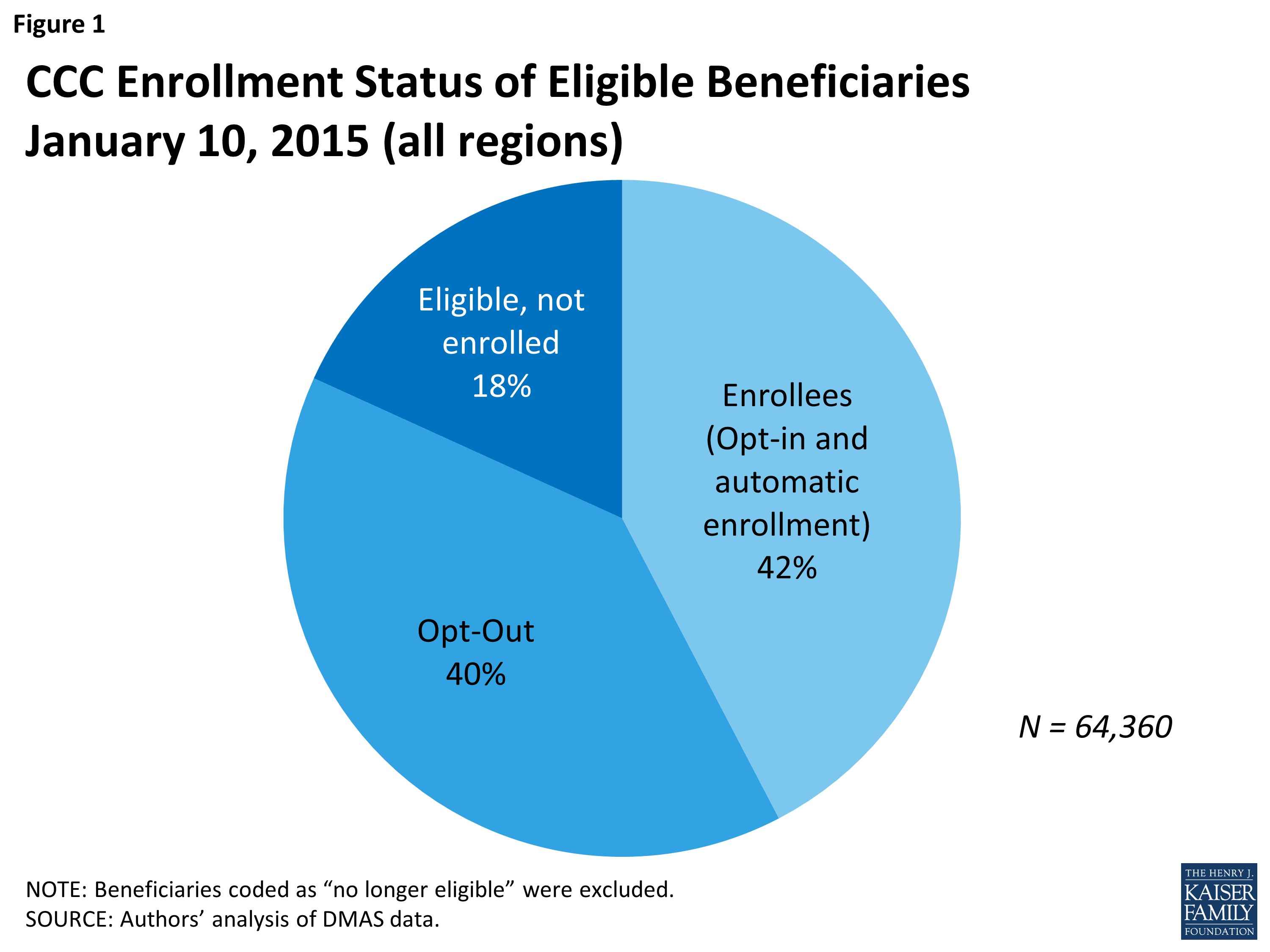
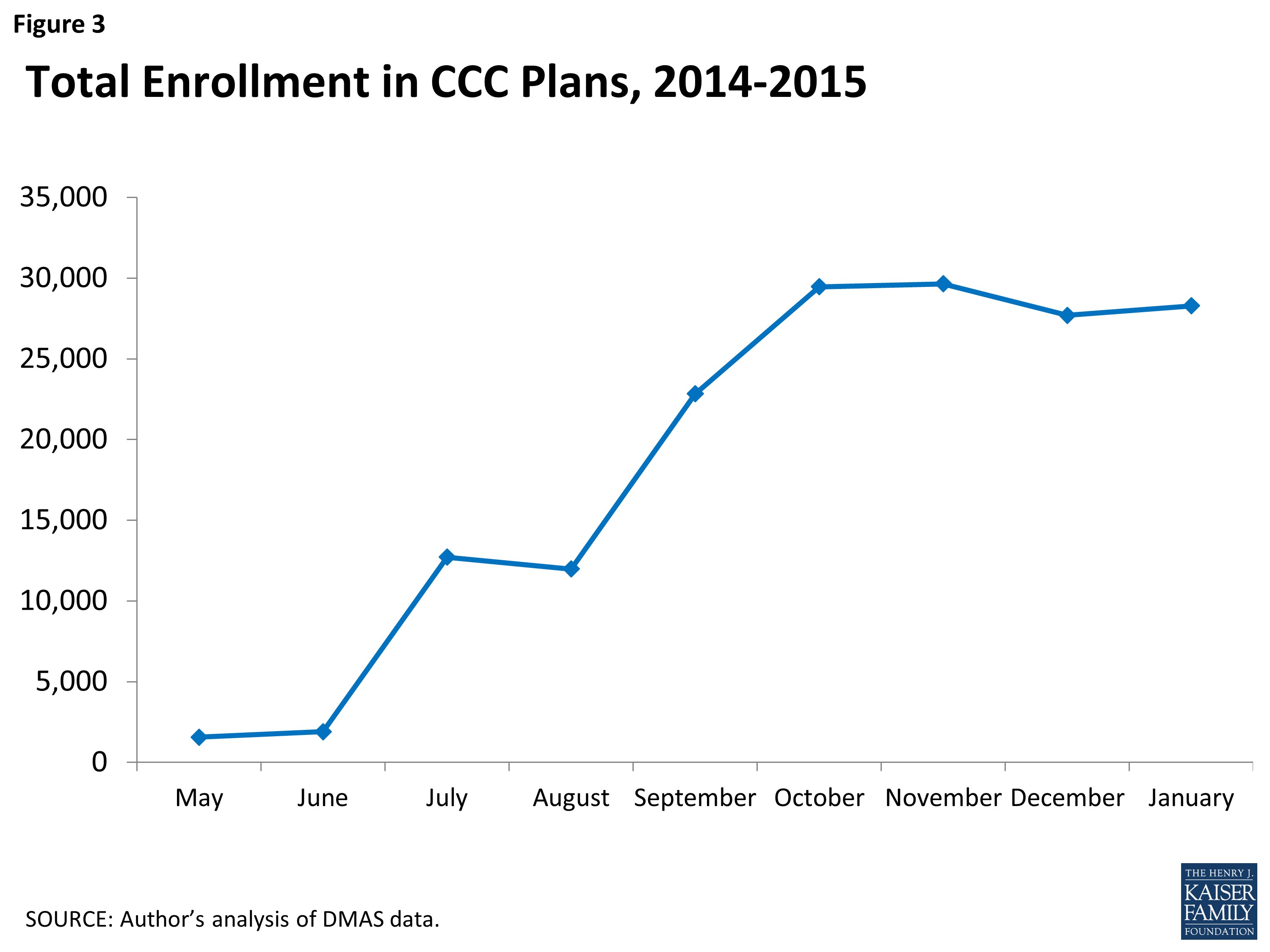
Program Enrollment Statistics: As of January 10, 2015, the CCC program had enrolled 27,333 beneficiaries across the five regions, representing approximately 42 percent of the eligible population. Another 40 percent of eligible beneficiaries had opted out of the program. The remaining 18 percent were not yet enrolled, had not opted out, and had not been subject to automatic enrollment. 11 Overall enrollment gradually increased with each phase of automatic enrollment throughout 2014. However, following the final round of automatic enrollment in November 2014, enrollment experienced a slight decline as new opt-outs exceeded new opt-ins (Figures 1, 2, and 3).
Figure 1: CCC Enrollment Status of Eligible Beneficiaries January 10, 2015 (all regions). Alt text: Bar chart showing the enrollment status of eligible beneficiaries in the Commonwealth Coordinated Care program across all regions of Virginia as of January 10, 2015, categorized into enrolled, opted out, and not enrolled/not opted out.
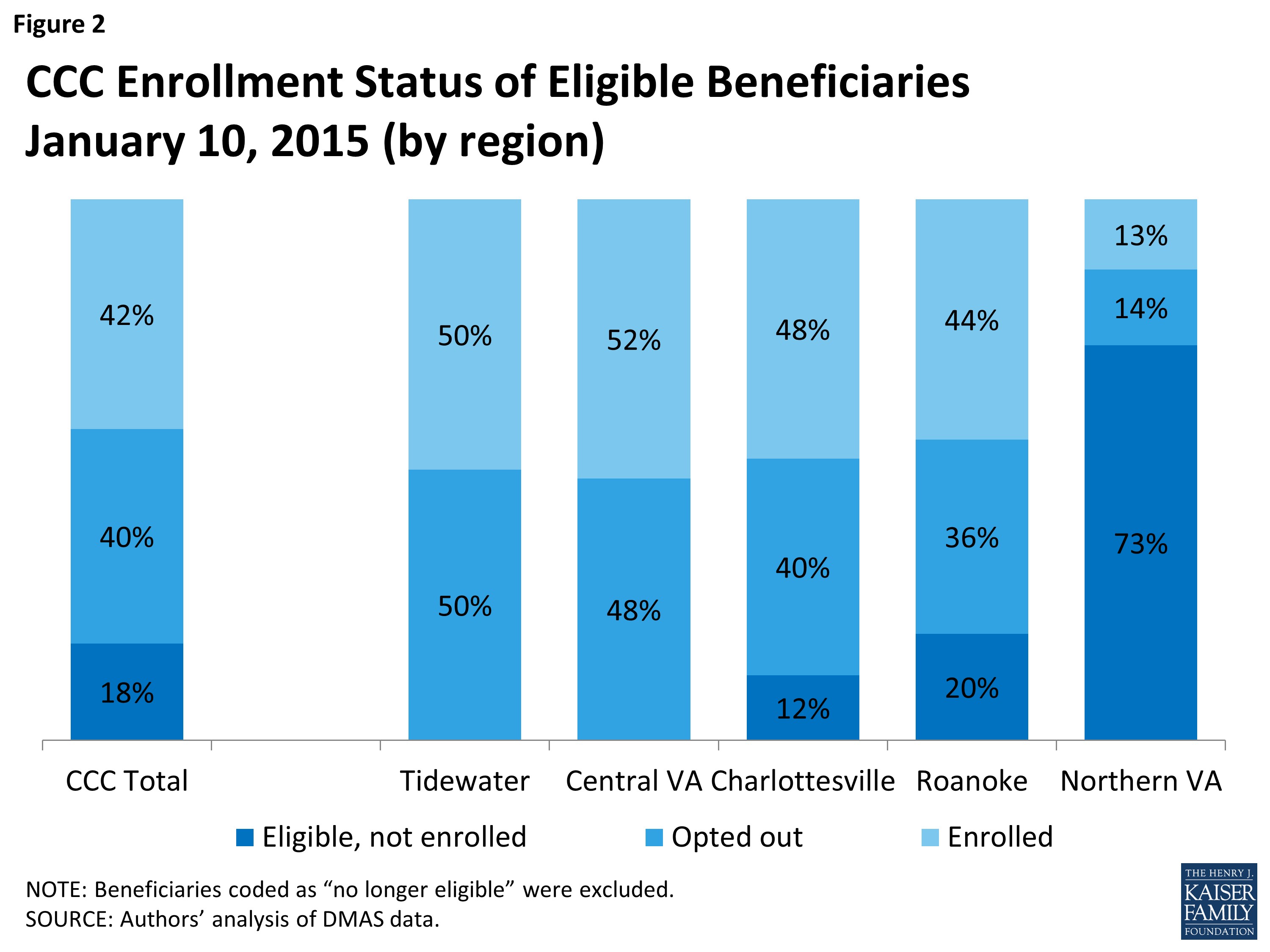
Figure 2: CCC Enrollment Status of Eligible Beneficiaries January 10, 2015 (by region). Alt text: Bar chart comparing the enrollment status of eligible beneficiaries in the Commonwealth Coordinated Care program across different regions of Virginia as of January 10, 2015, breaking down enrollment, opt-out, and not enrolled/not opted out rates for each region.
Figure 3: Total Enrollment in CCC Plans, 2014-2015. Alt text: Line graph illustrating the trend of total enrollment in Commonwealth Coordinated Care plans from 2014 to early 2015, showing the changes in enrollment numbers over time.
Automatic enrollment, and consequently overall program enrollment, lagged, particularly in certain areas of the state, due to several unforeseen complications:
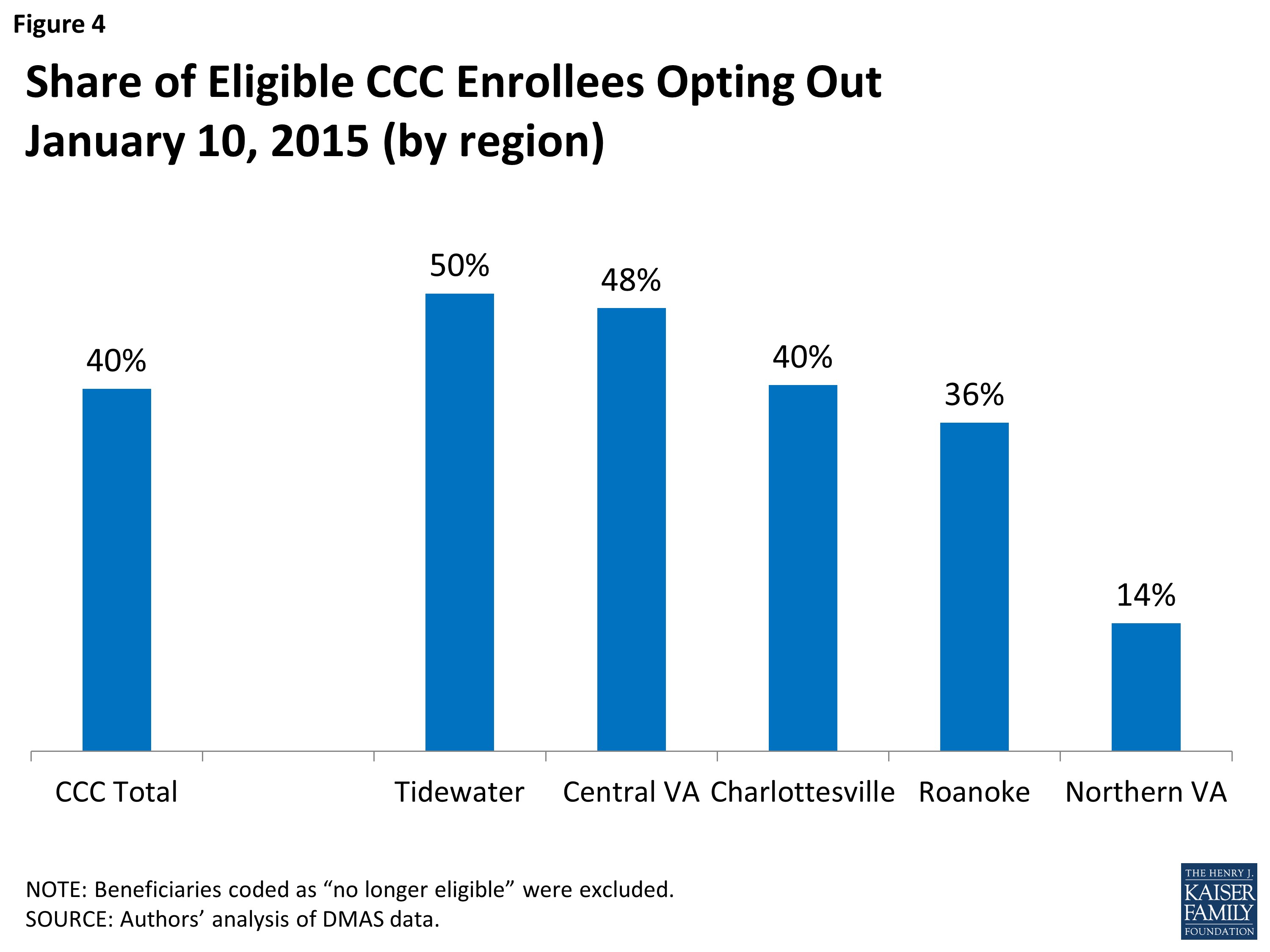
Program Opt-Out Rates: The opt-out rate in Virginia significantly influenced overall program enrollment. As of January 10, 2015, approximately 40 percent of all eligible beneficiaries had opted out statewide (Figure 4). In initial budget projections, Virginia officials had anticipated an 80 percent enrollment rate in CCC plans. 14 The observed opt-out rates resulted in enrollment figures considerably below these initial projections.
Figure 4: Share of Eligible CCC Enrollees Opting Out January 10, 2015 (by region). Alt text: Bar chart comparing the percentage of eligible Commonwealth Coordinated Care enrollees who opted out of the program across different regions of Virginia as of January 10, 2015, highlighting regional variations in opt-out rates.
Opt-out rates were notably higher in regions where automatic enrollment was implemented earlier (50 percent in Tidewater and 48 percent in Central Virginia) and substantially lower (14 percent) in Northern Virginia, where automatic enrollment had not been fully implemented in all localities. 15 The higher opt-out rates in more established regions likely reflect the program design that allows beneficiaries to opt out at any time. For example, in the Tidewater region, approximately one-quarter of the 11,900 beneficiaries who received the initial program letter opted out between receiving the letter and the scheduled enrollment date. A similar proportion opted out within their first three months as plan enrollees. Consequently, only 50 percent of beneficiaries initially notified about automatic enrollment were actually enrolled three months after the scheduled enrollment date. This pattern appeared consistent across cohorts with later enrollment dates, although complete data was not available at the time of this study. The overall opt-out rate could potentially increase as beneficiaries who were automatically enrolled had more time to evaluate their options.
Opt-out rates were significantly higher for beneficiaries participating in the EDCD waiver (receiving LTSS at home) compared to other groups. Nearly two-thirds of EDCD beneficiaries opted out. In contrast, opt-out rates for nursing facility residents and those living in the community without LTSS were similar to the program-wide opt-out rate.
Data collected by the enrollment broker indicated that the majority of beneficiaries who opted out cited satisfaction with their existing Medicaid and Medicare coverage. A smaller, yet significant, group opted out because their current healthcare providers did not participate in the program. 16 Given the slower-than-anticipated provider recruitment and the compressed implementation timeline, beneficiaries had to assess provider participation in the CCC program while plans were still actively contracting with providers. This situation contributed to confusion and concern among beneficiaries, posing an enrollment challenge.
Respondents also indicated that provider wariness of the new program influenced beneficiary enrollment decisions, with some nursing facilities initially attempting to opt out all of their eligible residents. State officials responded with a Medicaid memo clarifying beneficiary choice in the CCC program and initiated various provider education and engagement activities.
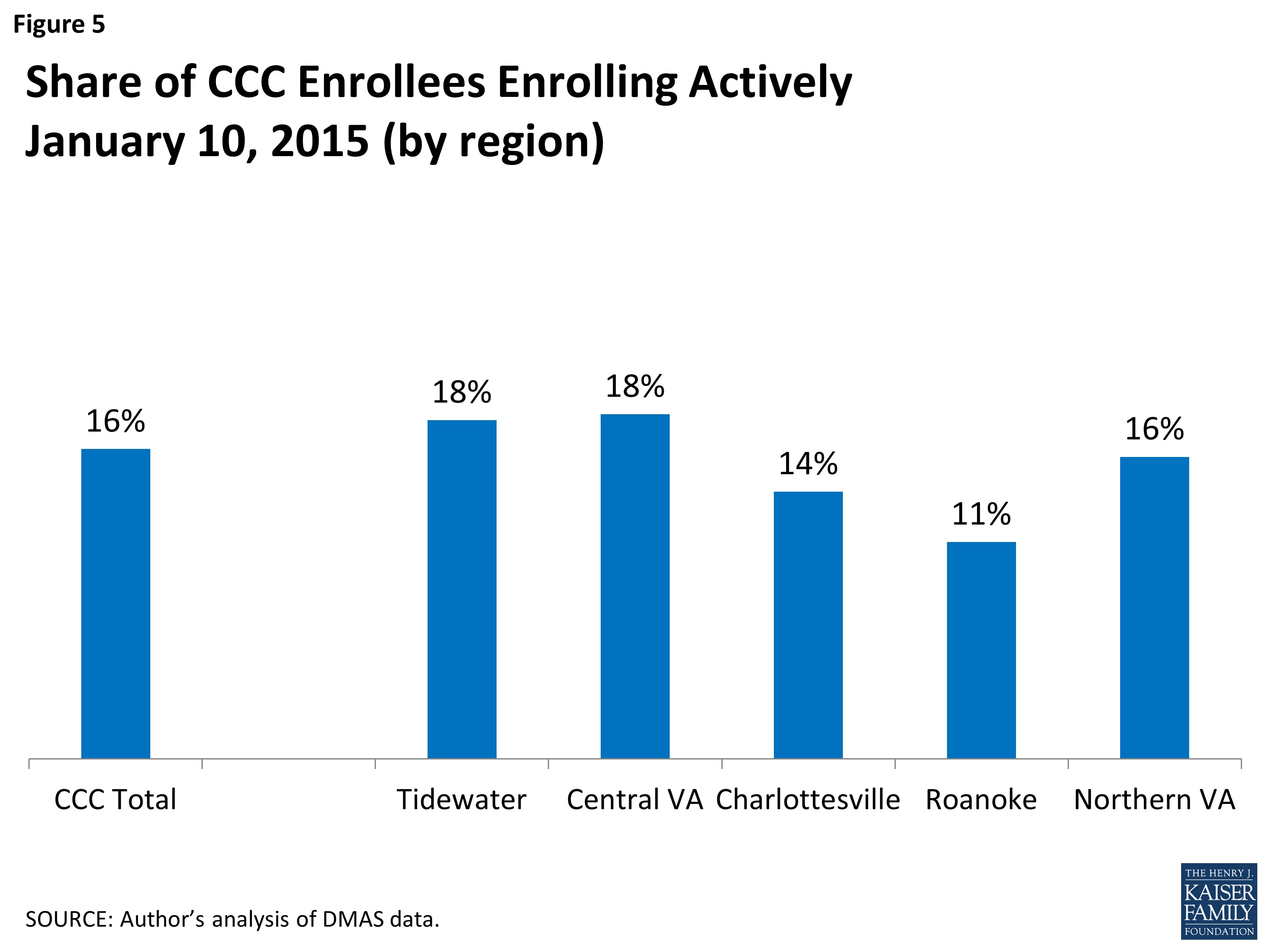
Program Opt-In Rates: The proportion of beneficiaries who proactively chose a CCC plan, as of January 10, 2015, was only 16 percent of total CCC enrollees and remained consistent across all regions (Figure 5). The remaining enrollees were automatically enrolled into their respective plans.
Figure 5: Share of CCC Enrollees Enrolling Actively January 10, 2015 (by region). Alt text: Bar chart showing the percentage of Commonwealth Coordinated Care enrollees who actively enrolled in the program, broken down by region in Virginia as of January 10, 2015, illustrating active enrollment rates across different regions.
While the demonstration did not mandate extra benefits beyond those required by Medicaid and Medicare, stakeholders reported that some beneficiaries who actively opted into the program were attracted by additional plan benefits. These included enhanced dental and vision services, podiatry care, gym memberships, and hearing exams and hearing aids. Others valued the potential for improved care coordination offered by the program.
Enrollment Volatility: All beneficiaries retained the right to join or leave the program in any month and to switch between the three available plans. Data provided to DMAS by the enrollment broker indicated that approximately two-thirds of beneficiaries who disenrolled cited a desire to return to their original coverage or the non-participation of their current provider in the program. Most of the remaining disenrollees expressed dissatisfaction with the program, the MMP, or the change in their coverage. 17 Understanding the reasons for disenrollment was a priority for CCC program staff, informing strategies to re-engage disenrolled beneficiaries. The state collected disenrollment reason data from plans and the enrollment broker, as well as through focus groups and surveys conducted as part of the state-sponsored evaluation.
Stakeholders identified confusion as a primary driver of enrollment changes, noting that many beneficiaries were initially unaware of their coverage transition. Both beneficiaries and providers who were aware of the program initially struggled to understand its implications and their respective roles.
Data from DMAS provided insights into the frequency of beneficiary movement in and out of the program and plan switching. As of January 2015 (approximately nine months after initial enrollments), around 2.6 percent of enrollees had switched plans. Additionally, about 1.5 percent of enrollees had opted back into the program after initially opting out. Most of the latter group rejoined after being automatically assigned to a plan by the state.
Stakeholders raised concerns about enrollment volatility and identified early issues related to enrollment changes:
- The state encountered limitations in fully testing information exchange systems with Medicare before program launch. Delays in information exchange between Medicare, Medicaid, MMPs, and the enrollment broker resulted in providers lacking real-time beneficiary enrollment status information. This uncertainty affected payment processes and service delivery. For example, nursing facilities experienced difficulties determining their residents’ plan enrollments. An eligibility system enhancement implemented in September 2014 improved provider access to beneficiary CCC program and plan enrollment information.
- Initially, some beneficiaries who disenrolled from the CCC program were unaware of the need to re-enroll in a Medicare Part D plan to restore their prior prescription drug coverage. While Medicare provided temporary safety net coverage, beneficiaries still needed to actively re-enroll.
- Plan switching created challenges in conducting comprehensive health assessments, developing effective care plans, and ensuring consistent service coordination.
Stakeholders expressed concerns about the long-term stability and viability of the CCC program if high opt-out rates or excessive plan switching persisted. Some suggested implementing a “lock-in period,” even for a short duration, or limiting the number of enrollment changes or plan switches within a year. However, they also acknowledged the need to balance these policies with protecting beneficiaries’ right to make coverage changes.
Respondents also highlighted potential coverage instability arising from beneficiaries failing to complete periodic Medicaid eligibility redetermination processes. Lapses in Medicaid eligibility would also result in CCC program ineligibility, even temporarily. They suggested that initiatives to ensure continuous coverage could be crucial for achieving program goals.
Health Plan Participation and Network Adequacy
Plan Participation in the CCC Program: In April 2013, Virginia initiated a health plan application process aiming to select at least two plans in each of the five program regions. Ultimately, three plans were selected, committing to serve beneficiaries across all five regions, contingent on plan readiness.
Program administrators deliberately chose a limited number of plans to streamline contract negotiations, simplify monitoring, minimize the number of plans providers needed to engage with, and foster collaboration among participating plans. Stakeholders agreed that having no more than three plans offered beneficiaries meaningful choices while simplifying the plan selection process compared to scenarios with a larger number of options.
As detailed in Table 2, only one of the selected plans had prior experience with both Medicare and Medicaid managed care in Virginia. However, their managed care experience in Virginia largely excluded dual-eligible beneficiaries. 18 Anthem HealthKeepers and Humana leveraged experience from their parent organizations in other states, including their Medicare Advantage Special Needs Plans for dual-eligible beneficiaries (dual SNPs). Both operated dual SNPs in Virginia, but Humana’s plans had limited enrollment statewide (approximately 1,000 enrollees), and Anthem’s plan had minimal enrollment.
| Table 2: Characteristics of the Three MMPs Participating in Virginia’s CCC Program |
|---|
| Plan |
| Anthem HealthKeepers |
| Humana Gold Plus Integrated |
| Virginia Premier Complete Care |
| SOURCES: Medicare Advantage and CCC enrollment from CMS administrative files. Medicaid enrollment from http://www.dmas.virginia.gov/Content_atchs/mc/mc-mcc2.pdf. |
In practice, all three plans participated across the five regions, though not in every city or county. Provider network gaps were particularly pronounced in certain locations, where prominent providers were hesitant to affiliate with plans. For instance, in some larger cities and counties in Northern Virginia, only one of the three plans had secured approval for an adequate provider network. Negotiations with health systems posed challenges for the other two plans in that region. With only one approved plan, beneficiaries could opt into the CCC program, but automatic enrollment was not possible. 19
Provider Networks within Plans: Developing robust provider networks for the CCC program presented a significant challenge for all participating plans. CCC plan networks required a broader range of service providers compared to typical Medicare, Medicaid, or private health insurance plans. The service spectrum encompassed traditional medical services, behavioral health services, and LTSS. State requirements for network adequacy were based on existing Medicaid and Medicare regulations, generally adhering to the more stringent of the two sets of rules.
Respondents highlighted various challenges in provider network recruitment. Anthem HealthKeepers and Humana could leverage their existing networks for Medicare Advantage services. Similarly, Anthem already had contracts with some Medicaid service providers. Virginia Premier benefited from its affiliation with the VCU Medical Center, providing a provider base, although this health system did not have reach across all regions. Virginia Premier also had established provider networks through its Medicaid managed care plan.
Building LTSS provider networks posed a particular challenge in the program’s early stages. Medicaid historically paid LTSS providers on a fee-for-service basis in Virginia, resulting in limited experience with managed LTSS. LTSS providers were encountering new policies and procedures, creating a steep learning curve. MMPs also faced a learning curve as they negotiated with new entities, including small business owners, and developed an understanding of the roles of community-based providers like Area Agencies on Aging or Centers for Independent Living. Some stakeholders suggested that plans might have had limited incentive to engage with a large number of smaller providers.
Certain program features facilitated provider network development. All plan contracts included an “any willing provider” policy for nursing facilities, ensuring nursing facility inclusion in plan networks as long as they accepted standard contract terms. Additionally, plans were mandated to pay nursing facilities at the same Medicaid rates used by the state. Plans were also required to contract with Community Service Boards, the public entities providing behavioral health services. Furthermore, all three plans had to utilize the same fiscal agent for consumer-directed services. The state established provider payment timeframes, and plans were required to regularly report claims turnaround times to the state. 20 Stakeholders generally reported that providers were paid promptly.
Cooperation and Communication: Respondents emphasized frequent communication and a “culture of cooperation” between CCC staff and MMPs, as well as among the three plans themselves. Most stakeholders interviewed, including those who raised program requirement concerns, praised state officials for their openness and outreach efforts. Plans jointly sponsored provider training meetings with provider organizations and developed common forms and procedures, such as for prior authorization. The state facilitated quarterly stakeholder meetings. Stakeholders noted that state staff were readily available to address individual problems. One challenge mentioned by a few respondents was leadership turnover within MMPs during the CCC program’s early phase.
Provider Perspectives and Engagement
Providers across various sectors generally expressed support for the CCC program’s objectives, particularly the emphasis on enhanced services and improved service coordination. However, some continued to have concerns regarding specific program details. Providers, especially those unfamiliar with managed care plans, exhibited some wariness towards the CCC program and the perceived “extra layer” of administration represented by MMPs. Recruiting providers for plan networks and educating them about new policies and procedures posed initial challenges. Providers were particularly concerned about payment processes, payment timeliness, and service authorization procedures. Traditional Medicaid medical service providers, such as physicians and hospitals, generally had greater familiarity with managed care. Behavioral health and LTSS providers had less prior experience with managed care at the program’s outset. Some providers expressed positive views of the new arrangement, recognizing the potential of aligned financial and clinical incentives within the CCC program to facilitate enhanced service delivery beneficial for their patients.
Early Program Impact on Providers: Larger provider organizations generally possessed greater capacity to adapt to new program requirements, although some reported needing to expand administrative functions to accommodate new procedures. Smaller, “mom and pop” providers, particularly LTSS providers who previously primarily interacted with Medicaid and sometimes Medicare, faced more significant challenges with new administrative demands related to credentialing, service authorization, and claims submission. These providers now had to navigate up to five entities – Medicaid, Medicare, and the three MMPs – each with distinct requirements and procedures, as some of their clients were in the demonstration while others were not.
Some providers lacked the infrastructure for electronic billing and payment and had not yet developed the capacity to bill plans electronically. Providers reported inconsistencies in billing and authorization procedures between fee-for-service Medicaid and Medicare and the MMPs. For example, they might need to utilize both electronic portals and paper forms. Authorizations could be required online or via telephone. These procedural variations caused confusion, especially during beneficiary transitions into or out of the CCC program. While a program goal was to streamline administrative processes for beneficiaries, processes became more complex for some providers as they navigated the requirements of each of the three plans.
Stakeholders emphasized the need for clarity regarding Medicaid, Medicare, and CCC policies that were not always aligned, particularly during beneficiary opt-in or opt-out events. For instance, Medicare’s 100-day limit on skilled nursing facility benefits contrasted with CCC plans’ flexibility to set different limits. Uncertainty existed regarding applicable rules when a patient receiving skilled care opted into or out of the CCC program while remaining in the same nursing facility. Providers also expressed confusion about the Medicare three-day qualifying hospital stay requirement for skilled care, which was waived for the CCC program but reapplied if a beneficiary opted out. Hospital readmission rules also differed across settings. Nursing facilities raised concerns about the implications of new CCC plan service delivery approaches for Medicaid and Medicare survey and certification reviews.
When unanticipated questions arose early in the program regarding the intersection of Medicaid, Medicare, and CCC policies, respondents noted that the clarification process was sometimes lengthy. One stakeholder observed that Medicaid and Medicare operations were not always synchronized, stating, “In reality, they are still two separate programs.” Respondents highlighted the steep learning curve for state officials and stakeholders unfamiliar with Medicare processes, noting that program staff often required input from CMS to resolve policy questions. Resolving policy questions requiring inter-office communication within CMS could be time-consuming. One respondent suggested that establishing a direct contact within the CMS Medicare office could be beneficial.
Several providers acknowledged that many initial challenges were related to program start-up and expressed optimism that the program would function smoothly once outstanding issues were resolved and stakeholders became more familiar with new program operations. Even at this early stage, some providers noted positive experiences working with plans, citing their responsiveness in resolving issues. One provider reported a shift in the “we-they” dynamic between providers and insurers, noting that in the new program, “things (such as obtaining equipment) happen quicker for patients.”
Provider Engagement Initiatives: The CCC program implemented extensive education and training efforts for providers, both initially and on an ongoing basis. Early in the program, private foundations supported provider training for nursing facilities, personal care providers, and service facilitators. As program rollout progressed, program and plan staff recognized the need for more intensive support, particularly for smaller providers, to navigate the new operational landscape. The CCC program sponsors ongoing provider outreach and training, including regional town halls and on-site training upon request. Weekly calls are also conducted for five provider types: adult day service providers, personal care and home health service facilitators, nursing facilities, hospitals and medical practices, and behavioral health providers. Six months after the initial enrollment date, program staff noted that providers were at varying stages of CCC program understanding, and provider education remained a significant focus.
Service Delivery and Care Coordination
Initial Health Risk Assessments (HRAs): MMPs were required to conduct Health Risk Assessments (HRAs) for all new enrollees within 90 days of enrollment. For enrollees categorized as “vulnerable subpopulations,” the assessment timeframe was shortened to 60 days. 21
HRAs served as the foundation for developing individualized care plans, specifying the types and amounts of services beneficiaries would receive. Plans were mandated to conduct face-to-face assessments for nursing facility residents and EDCD waiver enrollees. Assessments for other enrollee categories could be conducted via telephone. Providers emphasized the importance of in-person assessments for patients with complex conditions and high needs, conducted in their homes rather than remotely. Assessment backlogs appeared to be linked to the program’s ambitious start-up schedule. The phased enrollment schedule helped manage the volume of HRAs required at any given time. However, automatic enrollment led to large cohorts of beneficiaries in each region being assigned to plans on the same effective date, creating assessment workload peaks.
Another factor affecting plans’ HRA completion capacity was incomplete contact information for some automatically enrolled beneficiaries. This not only complicated HRA scheduling but also indicated that some auto-enrollees might not have received program information and would require program explanations alongside assessments. A promising practice adopted by plans was utilizing pharmacy records, when available, to help locate beneficiaries. Monthly prescription refills often represented the first contact point between enrollees and their new plans.
At this stage of program implementation, it was challenging to determine the extent to which HRAs had resulted in care plan modifications or their perceived value by enrollees and providers. Plan staff noted that HRAs provided opportunities to identify under-reported behavioral health needs, initiate disease management referrals, and plan care for high-cost, high-need members. Observers were not aware of service reductions linked to initial assessments and subsequent care plans. Each MMP documented success stories illustrating the role of assessments in improving enrollee care. However, generalizing from these anecdotes was not feasible.
The assessment and care planning processes also provided a platform to discuss beneficiaries’ interest in self-directing certain services, such as personal care attendant services. Stakeholders reported that plans were in the early stages of facilitating beneficiary self-direction.
Continuity of Services and Providers: Maintaining continuity of care during beneficiaries’ transition from traditional Medicaid and Medicare to MMPs was a central program priority. This transition period also served as a timeframe for providers and MMPs to complete credentialing and contracting processes for providers not initially included in plan networks. Plans were required to allow new CCC enrollees to maintain their current providers (including out-of-network providers) and pre-authorized services for 180 days from initial enrollment. Enrollees transferring from another MMP could maintain current providers and pre-authorized services for 30 days. Nursing facility residents were permitted to remain in their current facility for the demonstration’s duration, as long as they continued to meet nursing facility care criteria, even if the facility was not part of their plan’s network. 22 These policies aimed to ensure seamless care transitions for beneficiaries. 23
Limited issues related to continuity of care were apparent in the program’s early stages, as the transition period was still active for most enrollees. However, respondents identified implementation considerations:
- Transition protections might mask underlying provider network inadequacies that could emerge later.
- Beneficiaries unaware of coverage changes might be surprised at the end of the transition period when needing to find new providers.
- Lack of familiarity with transition policies was cited as a reason some providers discouraged beneficiaries from CCC program participation. Providers were not aware of continued payment for services during the transition, payment procedures, or the option for “single case agreements” allowing enrollees to continue with out-of-network providers.
Service Access and Enhanced Benefits: Given the ongoing transition period for most enrollees, it was premature to fully assess service access issues. The enhanced services and benefits offered by CCC plans were a particularly attractive program feature. Stakeholders reported early instances of beneficiaries encountering access issues related to these services. Improved access to behavioral health services was another appealing program aspect. For example, nursing facilities anticipated improved behavioral health options and services for residents. Health plans were collaborating with Virginia’s Community Services Boards to develop behavioral health homes, aiming to better coordinate care for CCC enrollees with serious mental illness. Plans for these service enhancements were progressing, but early indications suggested limited implementation at the time of this study.
The promise of enhanced access to community-based LTSS was another area of significant interest. Plans had greater flexibility in service provision. There was an expectation that program costs could be reduced while improving quality by enabling more beneficiaries who utilized LTSS to live independently in the community rather than in institutional settings. Respondents questioned whether community-based service utilization would be substantial in Virginia, given stricter Medicaid LTSS eligibility criteria compared to other states. Other key issues raised included community housing availability, workforce adequacy to support community-based LTSS, and MMPs’ capacity to contribute to building this capacity.
Program policies mandated provider accommodation of enrollees with disabilities, ensuring facility accessibility and flexible appointment scheduling. Plans and providers were also required to effectively communicate with individuals with hearing impairments, limited English proficiency, or cognitive impairments. Program effectiveness in these areas remained to be determined at the time of the study.
Service Coordination and Care Management: Service coordination was widely recognized as a highly desirable CCC program feature. One provider noted that the program would enable their organization to emphasize comprehensive healthcare delivery. Notable early improvements included enhanced round-trip transportation services offered by one plan and the development of an electronic record access system to improve care coordination for patients with behavioral health and medical conditions. Other coordination activities included facilitating hospital discharge transitions to appropriate settings and medication management support. Anecdotal reports from MMPs highlighted care manager efforts to identify depression signs, arrange appropriate care, assist enrollees and families with end-of-life decisions, and arrange personal emergency response systems and home renovations to support independent living at home.
Care or service coordination generally encompasses non-clinical functions like information provision, logistical support, timely patient information transfer, and referral/transition tracking to address process gaps. Case management often involves more intensive services provided by nurses or other health professionals to high-risk patients. 24 Stakeholder confusion existed regarding communication and collaboration between different types of care coordinators and managers, and the impact on beneficiaries and providers. Prior to CCC enrollment, beneficiaries might have worked with social workers in primary care settings or institutions or received Medicaid targeted case management services. Post-enrollment, plan care coordinators or managers became involved.
Notable early instances of organizational collaboration emerged. Area Agency on Aging staff, traditionally providing fee-for-service care management, were now offering these services for at least one plan. A large primary care practice allocated space within their facility for MMP case managers to work on-site, facilitating improved communication with provider care teams.
MMPs were required to establish Interdisciplinary Care Teams (ICTs), and the program aimed to promote behavioral health home creation in partnership with Community Services Boards for enrollees with serious mental illness. Respondents reported initial plan staff engagement in these areas but noted that it was too early to evaluate the impact on providers or enrollees. One provider perceived that “at this point, ICTs really only exist in theory.”
Performance Assessment and Quality Measures
All respondents concurred that it was too early to definitively assess the CCC program’s achievement of its ambitious goals. At the six-month mark, stakeholders suggested that at least one to two years post-program launch would be necessary to move past initial start-up challenges and begin to evaluate program success. However, DMAS was actively engaged in monitoring program operations, addressing identified issues, and making adjustments to optimize program functionality.
Demonstration Oversight Mechanisms: Robust oversight was a key feature of the CCC program. Plans were required to submit weekly “dashboards” – operational data reports – to DMAS and CMS. Required data included opt-in/opt-out enrollment numbers, outreach calls and home visits to new members, completed HRAs and care plans, and new, open, and closed appeals. Plans also reported on frequent enrollee and provider call topics, provider training activities, provider networks, and claims processing times. Program staff conducted weekly contract monitoring team meetings with each plan.
CCC staff proactively made program adjustments based on feedback. For example, in response to provider reports of confusion during beneficiary disenrollment and return to traditional Medicaid or Medicare, DMAS extended the timeframe for continuity of care authorizations upon return to fee-for-service. System enhancements were also implemented to improve access to Medicaid beneficiary eligibility status information, including CCC program and MMP enrollment details.
Quality Measurement Framework: Virginia developed a comprehensive list of 113 core quality measures for the demonstration. This included 71 CMS-specified measures, 32 measures primarily related to LTSS already used for the EDCD waiver, and 10 measures specifically developed for the CCC program. New measures focused on areas like tracking demographic data, documenting care goals, monitoring LTSS service authorization changes, and tracking LTSS enrollee transitions between community-based and institutional settings. Subsets of core quality measures were designated as “quality withhold measures.” Each year, the state and CMS withheld a percentage of capitation payments, contingent on plan performance against these measures. Respondents, particularly from plan and provider communities, acknowledged the importance of quality measurement but expressed concerns about the sheer volume of measures and the reporting burden.
Stakeholder Engagement and Transparency: DMAS actively analyzed and publicly presented program data in a timely manner at quarterly stakeholder advisory committee meetings, other forums, and on the program website. Plans were required to establish independent beneficiary advisory committees, providing input to governing boards and including beneficiaries with disabilities in plan governance structures. Each plan held initial advisory committee meetings in June 2014. Stakeholders considered it too early to assess the impact of these committees.
Ombudsman Office Role: The state secured a federal grant to support a new full-time staff position to expand the state long-term care ombudsman’s capacity to address community-based LTSS issues. A notable feature was the ombudsman office’s operational independence from the CCC program, although it remained a state government entity. 25 Publicizing ombudsman assistance required extra effort. Early in the program, the office’s role and availability were not widely known within the stakeholder community. Most of the 46 cases handled by the CCC ombudsman between June and late October 2014 involved plan authorization assistance for enrollees or providers, enrollment/disenrollment problems, Part D prescription drug coverage, or service access issues. 26
Program Evaluation Initiatives: In addition to participating in a national CMS-sponsored demonstration evaluation, DMAS and researchers at George Mason University were conducting a state-specific evaluation. This included site visits and focus groups to gather insights into beneficiaries’ early program experiences. A telephone survey of personal care service enrollees was also planned. Evaluators collaborated with community-based groups like Centers for Independent Living, Area Agencies on Aging, and Community Services Boards to recruit focus group participants. Preliminary focus group findings indicated that beneficiaries viewed enhanced benefits, care coordination, and customer service as positive CCC program features. Identified concerns included enrollment system errors, personal care attendant authorizations and payments, narrow provider networks, and prescription coverage issues. 27
Program Financing and Savings Projections
State officials projected that efficiencies achieved through the CCC program would generate financial savings for Virginia. The agency’s fiscal year 2014 budget forecast included total savings of $44 million for 2014-2016 (split equally between general funds and federal matching funds) attributed to the demonstration. 28 This projection assumed an 80 percent enrollment rate in CCC plans. The state projected $28 million in savings with a 50 percent enrollment rate. Capitation rate reductions paid to health plans were the primary mechanism for achieving savings. In January 2015, state officials revised the savings projection for fiscal years 2015-2016, reducing the estimate by $10 million in general funds ($20 million total), likely reflecting lower-than-expected enrollment.
Many stakeholders recognized the potential for cost reduction through the CCC program, citing potential reductions in unnecessary hospitalizations or emergency department visits and improved care coordination. However, stakeholders cautioned that it was essential to understand whether savings stemmed from improved service delivery or simply service reductions. Respondents anticipated that achieving savings would take at least a year. Furthermore, some noted that upfront investments by plans and providers to develop improved care delivery models might be necessary before savings could materialize.
CCC health plans received capitation payments for each enrolled member, covering all services for CCC beneficiaries. Capitation payments comprised three components: a payment from Virginia based on historical fee-for-service payments, a CMS payment for Medicare Parts A and B services, and a separate CMS payment for Medicare Part D prescription drug services. 29 Medicare payments followed standard Medicare Advantage and Part D plan payment methodologies, adjusted for member health status using Medicare’s risk adjustment methodologies.
Virginia’s Medicaid payments were based on historical fee-for-service Medicaid payments. The state used 2011-2012 payment claims to estimate costs in the absence of the CCC program. These costs were adjusted to reflect benefit changes and spending trends between 2011-2012 and the demonstration period. Base Medicaid rates were set separately for each of the five CCC program regions and risk-adjusted based on member rate cells. Four rate cells were used, based on age (21-64 and 65+) and nursing facility level of care criteria (EDCD waiver enrollment or nursing facility residence for 20+ consecutive days). LTSS enrollees were designated as “nursing home eligible” or “community well.” 30 Rate cells did not account for health conditions or service needs. This rate cell structure meant plans received the same Medicaid payment for “community well” enrollees, regardless of health status or chronic conditions. Monitoring the impact of these payment policies on ensuring appropriate care for all enrollees was crucial.
Plans received the same Medicaid payment for all LTSS enrollees, whether in the community or nursing facilities, creating an incentive for community-based care, generally less costly per person. 31 Plans received a temporary enhanced rate for two months after an enrollee transitioned from nursing home eligible to community well status. Understanding the impact of this policy on level of care designation changes during nursing facility eligibility redeterminations was important.
As outlined in the Memorandum of Understanding between Virginia and the federal government, Medicaid and Medicare Parts A/B capitation payments (excluding Part D) incorporated savings percentages: 1% in year one, 2% in year two, and 4% in year three. These reductions aimed to capture savings from improved Medicare-Medicaid service coordination. A limited risk-sharing provision was included to protect plans. In year three, the savings percentage would be lowered from 4% to 3% if any of the three plans experienced losses exceeding 3% of revenue in year one across all regions (based on 20-month data from February 2014 to December 2015).
In addition to savings reductions, quality withholds were implemented: 1% in year one, 2% in year two, and 3% in year three, applying to state Medicaid and Medicare Parts A/B payments (excluding Part D). Federal and state agencies evaluated plan performance against a set of measures to determine if plans earned back the quality withhold each year. Eight measures were specified for year 1, and 12 measures for subsequent years. Examples included documented care plans within timeframes, care plan discussions of care goals, and smooth hospital/nursing facility/community transitions.
Participating CCC plans were also subject to a minimum medical loss ratio requirement – the percentage of total payments covering medical claims and enrollee care/quality expenses. Plans not achieving a 90% loss ratio faced corrective action plans, with fines for loss ratios between 85-90%. Loss ratios below 85% required plans to return a portion of payments. These provisions aimed to limit plan administrative costs and profits, ensuring that most payments directly benefited enrollees.
Looking Ahead and Program Sustainability
Respondents emphasized that the CCC program’s long-term viability depended on attracting and retaining beneficiary enrollment. Some suggested exploring restrictions on program opt-outs or plan switches, while others raised concerns about limiting beneficiary choice. They recommended assessing beneficiary opt-in/opt-out and plan switching patterns post-transition before proposing policy changes. Unlike demonstrations in some other states, Virginia allowed beneficiaries to opt out of the CCC program and remain in fee-for-service Medicaid. If this option were removed in the future, understanding the impact on beneficiaries and the program would be critical.
Respondents also underscored the link between robust provider networks and program sustainability. Plan decisions regarding network breadth, provider decisions on network participation, and beneficiaries’ desires to maintain current providers would all play significant roles. Stakeholders observed that beneficiary enrollment and retention were more likely if providers supported the program and beneficiaries could continue with their existing providers post-transition. Continued commitment to information, education, and training, along with timely policy clarifications from CMS, could enhance provider confidence in the program.
As more data becomes available, understanding the impact of HRAs on care plan changes and whether these changes resulted in service enhancements or reductions would be crucial. Service accessibility assessments and appeals process utilization and outcomes would also provide valuable insights.
It was premature to determine if the program would achieve its care improvement goals. Anecdotal reports from plans highlighted service delivery improvements for individual beneficiaries, but the broader extent of these improvements remained unclear. Respondents stressed the importance of assessing ongoing service coordination effectiveness and reviewing HRA and care plan data as it developed. Enrollment stability and care coordinator/case manager workforce stability were identified as factors influencing long-term service delivery quality.
Stakeholders also sought to understand the program’s impact on service costs for dual-eligible beneficiaries but cautioned that it was too early to assess savings. Understanding the drivers of any savings, such as improved coordination versus service reductions, and accounting for investments in service delivery improvements were essential.
Stakeholders generally expressed eagerness to move beyond initial start-up issues. The post-transition period would be critical for understanding the program’s impact on beneficiaries and its long-term effects.
This issue brief was prepared by Laura Summer and Jack Hoadley of the Georgetown University Health Policy Institute.
Executive Summary