
The escalating costs of healthcare in the United States demand innovative solutions that not only enhance patient care but also offer substantial financial benefits. Palliative care, particularly through hospital consultation programs, has emerged as a vital approach in achieving these dual objectives. While the primary focus of palliative care is to improve the quality of life for patients and their families facing serious illnesses, a growing body of evidence highlights the significant Cost Savings Associated With Us Hospital Palliative Care Consultation Programs. This article delves into these financial advantages, exploring how integrating palliative care consultations can lead to more efficient healthcare resource utilization and reduced overall expenditure.
Understanding the Financial Impact of Palliative Care Consultation
Palliative care is a specialized medical field focused on providing relief from the symptoms and stress of a serious illness. Unlike hospice care, which is for patients nearing the end of life, palliative care can be beneficial at any stage of a serious illness and can be provided alongside curative treatment. Hospital palliative care consultation programs involve a multidisciplinary team of experts — physicians, nurses, social workers, and chaplains — who collaborate with the patient’s primary medical team to offer an extra layer of support.
The economic benefits of inpatient palliative care consultation are becoming increasingly recognized. Traditionally, discussions around palliative care focused on ethical considerations and patient-centered outcomes. However, the financial realities of modern healthcare necessitate a closer look at the economic implications. Studies have consistently shown that palliative care consultation programs can lead to decreased healthcare utilization, particularly in resource-intensive areas such as inpatient hospital stays. This reduction in utilization directly translates into considerable cost savings associated with US hospital palliative care consultation programs.
One significant factor driving these savings is the alignment of care with patient preferences. Palliative care emphasizes advance care planning (ACP), a process that allows patients to articulate their wishes regarding medical treatment, especially at the end of life. By engaging in ACP, patients are more likely to receive care that is consistent with their values and goals, often leading to a reduction in aggressive, costly, and potentially unwanted medical interventions.
Patient cohort selection and matching.
Evidence from Research: Advance Care Planning and Cost Reduction
A pivotal study investigated the link between outpatient advance care planning (ACP) and healthcare costs and utilization within a large accountable care organization (ACO). This research provides compelling evidence for the cost savings associated with palliative care consultation programs, as ACP is often a critical component of such programs. The study employed a case-control design, comparing patients who engaged in ACP (cases) with matched controls who did not.
Study Design and Methodology
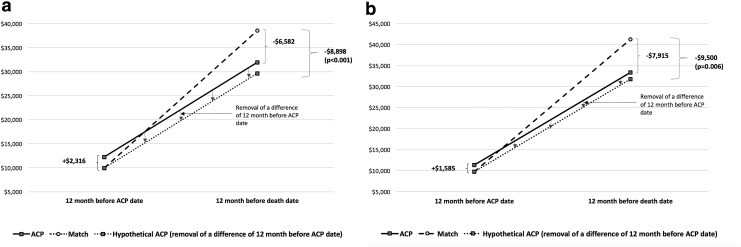
The study meticulously matched 325 patients who had participated in outpatient ACP with 325 control patients based on various demographic and clinical factors, including age, gender, race, comorbidity index, and predicted utilization risk. Data were collected from ACO records, an ACP facilitator database, and electronic medical records. The researchers analyzed healthcare utilization and costs for a 12-month period before ACP (for cases) or a matched date (for controls), and for the 12 months preceding death. A difference-in-difference analysis was used to account for pre-existing differences between the groups.
Key Findings: Cost Savings and Utilization
The results of this study are striking in demonstrating the cost savings associated with palliative care consultation programs, particularly those incorporating ACP. The adjusted analysis revealed that patients who underwent ACP experienced:
- Reduced Inpatient Admissions: The ACP group had significantly fewer inpatient hospital admissions compared to the control group (-0.37 admissions, 95% CI -0.66 to -0.08).
- Decreased Inpatient Days: ACP was associated with a notable reduction in inpatient hospital days (-3.66 days, 95% CI -6.23 to -1.09).
- Overall Cost Reduction: Adjusted healthcare costs were substantially lower in the ACP group, with an average savings of $9,500 per patient (95% CI -$16,207 to -$2,793).
Notably, the study found no significant differences in hospice use, skilled nursing facility use, home health use, or emergency department visits. This suggests that the cost savings were primarily driven by the reduced need for expensive inpatient hospital care.
Cost comparison. Costs were compared with a difference-in-difference method, using a generalized linear model with gamma distribution for expenditures (a) and a generalized linear model with gamma distribution adjusted by age, gender, race, CMS risk score, and comorbidities (CHF, COPD, ESRD, and cancer) (b). All expenditures were converted to 2016 U.S. dollars using the Medical Component of the Consumer Price Index. For patients (N = 190 and each group N = 95) who do not have a full 12-month period between ACP date and death date, we used a multiple imputation method. Ten imputed values were obtained for each missing observation with the mean used for the missing value. ACP, advance care planning; CHF, congestive heart failure; CMS, Center for Medicare and Medicaid Services; COPD, Chronic Obstructive Pulmonary Disease; ESRD, end-stage renal disease.
Advance Directives and Documentation
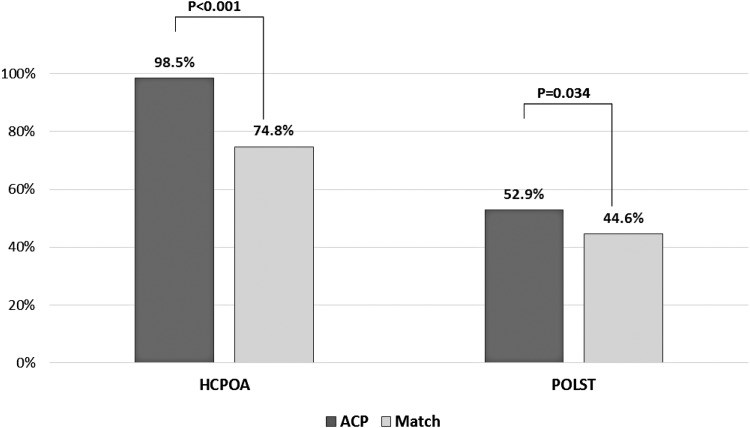
Beyond cost savings, the study also confirmed that ACP significantly increases the documentation of advance directives. A significantly higher proportion of ACP participants had a Healthcare Power of Attorney (HCPOA) (98.5% vs. 74.8%) and Practitioner Orders for Life-Sustaining Treatment (POLST) forms (52.9% vs. 44.6%) documented compared to the control group. This increased documentation ensures that patient wishes are known and respected, further contributing to patient-centered care and potentially avoiding unwanted interventions.
In the twelve months prior to death, the proportion of Health Care Power of Attorney (HCPOA) and Practitioner Orders for Life Sustaining Treatment (POLST).
The Broader Impact of Palliative Care Consultation Programs
While this study focused on ACP, its findings are highly relevant to understanding the broader cost savings associated with US hospital palliative care consultation programs. ACP is a core component of palliative care, and the principles of patient-centered communication, symptom management, and care coordination that drive cost savings in ACP are also central to palliative care consultation programs.
Reduced Hospital Readmissions
Palliative care consultation programs are designed to provide holistic care that addresses not just the physical symptoms but also the emotional, social, and spiritual needs of patients and their families. This comprehensive approach can lead to better symptom management, improved patient and family coping, and enhanced communication between patients, families, and healthcare providers. As a result, patients receiving palliative care are often less likely to experience complications or exacerbations of their conditions that would necessitate hospital readmissions. Reducing readmission rates is a key area where cost savings associated with US hospital palliative care consultation programs are realized, as readmissions are a significant driver of hospital expenditure.
Improved Patient Outcomes and Satisfaction
Palliative care is fundamentally about improving patient quality of life. By focusing on symptom relief, pain management, and psychosocial support, palliative care consultation programs can significantly enhance patient comfort and well-being. Patients who feel heard, understood, and supported are more likely to adhere to their treatment plans and experience better overall health outcomes. Furthermore, patient satisfaction is often higher in palliative care settings due to the emphasis on patient preferences and shared decision-making. While not directly a cost saving, improved patient satisfaction can lead to better reputation and patient retention for hospitals, which has long-term financial benefits.
Efficient Resource Allocation
One of the key mechanisms through which palliative care consultation programs generate cost savings is by promoting more efficient allocation of healthcare resources. By facilitating conversations about goals of care and prognosis, palliative care teams help ensure that patients receive care that is appropriate and aligned with their needs. This can lead to a reduction in the use of futile or overly aggressive treatments, especially for patients with advanced illnesses. Avoiding unnecessary procedures, tests, and prolonged hospital stays frees up resources that can be better utilized elsewhere in the healthcare system.
Return on Investment for Hospitals
Implementing and maintaining palliative care consultation programs requires investment. However, the evidence suggests a strong return on investment (ROI) due to the significant cost savings associated with US hospital palliative care consultation programs. The study highlighted earlier calculated an impressive ROI of 104% for their ACP program, demonstrating that the savings generated far outweighed the program costs, which included facilitator training, administration, and program start-up expenses.
This ROI calculation underscores the financial prudence of investing in palliative care. Hospitals that establish robust palliative care consultation services are not only enhancing the quality of care they provide but are also positioning themselves to achieve substantial financial benefits through reduced healthcare utilization and expenditure. In an era of value-based care, where healthcare providers are increasingly incentivized to deliver high-quality care at lower costs, palliative care consultation programs represent a strategic and ethical imperative.
Table 3.
Return on Investment
| 2013 | 2014 | 2015 | 2016a | Total | ||
|---|---|---|---|---|---|---|
| Cost of ACP | ||||||
| Education program cost ($)b | A | $43,980 | $42,932 | $56,791 | $18,237 | $161,941 |
| Number of ACPs done (person) | B | 4672 | 3985 | 4448 | 1489 | 14,594 |
| Weighted average cost per ACP ($)c | C | $29.54 | ||||
| Execution cost ($) | D = B × C | $431,107 | ||||
| Maintenance cost of program ($) | E | $120,054 | $159,047 | $155,015 | $49,282 | $483,398 |
| Start-up cost ($) | F | $438,724 | ||||
| Total ACP intervention cost ($) | G = A+D+E+F | $1,515,170 | ||||
| Benefit of ACP | ||||||
| Reduced expenditure of last 12 months of life per patient ($) | H | $9,500 | ||||
| Number of patients died (person) | I | 325 | ||||
| Total benefit of ACP intervention ($) | J = H × I | $3,087,500 | ||||
| ROI | ||||||
| Total cost ($) | K = G | $1,515,170 | ||||
| Net benefit (total benefit-total cost) ($) | L = J−K | $1,572,330 | ||||
| ROI | M = (L/K) × 100 | 104% |
a2016 is a partial year of January–April.
bEducation costs increased slightly with the addition of simulation.
cWeighted average costs reflect that the majority of ACPs were facilitated by nurses and social workers. ROI, return on investment.
Addressing Challenges and Future Directions
Despite the compelling evidence for cost savings associated with US hospital palliative care consultation programs, several challenges remain in widespread implementation and optimization. These include:
- Awareness and Access: Many patients and healthcare providers are still not fully aware of the benefits of palliative care, leading to underutilization of these services.
- Integration with Existing Care Models: Seamlessly integrating palliative care consultation into existing hospital workflows and specialties requires careful planning and coordination.
- Workforce Development: There is an ongoing need to train and support a sufficient number of palliative care professionals to meet the growing demand.
- Data Collection and Outcome Measurement: Standardized metrics and robust data collection systems are needed to further quantify the impact of palliative care programs on costs and outcomes across diverse settings and patient populations.
Future research should focus on addressing these challenges and further refining our understanding of the economic and clinical benefits of palliative care. Studies exploring the optimal timing of palliative care consultation, the most effective models of program delivery, and the long-term impact of palliative care on patient and family well-being are crucial for advancing the field.
Conclusion
The evidence is clear: cost savings associated with US hospital palliative care consultation programs are significant and well-documented. By reducing inpatient utilization, improving resource allocation, and aligning care with patient preferences, palliative care consultation programs offer a powerful strategy for simultaneously enhancing patient care and controlling healthcare costs. As the healthcare landscape continues to evolve, the financial and ethical imperatives for integrating and expanding palliative care services in US hospitals will only become more pronounced. Investing in palliative care is not just an act of compassion; it is a sound economic decision that benefits patients, families, healthcare systems, and society as a whole.
References
[1] Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life. Washington, DC: National Academies Press; 2014.
[2] Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. JAMA. 2008;299(20):2369-2377.
[3] Gillick MR. Palliative care should be part of mainstream medicine. JAMA. 2008;299(20):2437-2439.
[4] Lupu D, Maxwell C, Ohsfeldt RL. Public awareness and attitudes toward palliative care in the US. J Pain Symptom Manage. 2006;32(2):105-115.
[5] Teno JM, Gozansky WS, Weeks J, et al. Decision-making and outcomes of care in seriously ill hospitalized patients: does age matter? J Am Geriatr Soc. 1997;45(10):1217-1224.
[6] Emanuel LL, von Gunten CF, Ferris FD. Advance care planning: ensuring care consistent with patients’ values and preferences at the end of life. Ann Intern Med. 2000;132(12):1009-1014.
[7] Rietjens JA, Sudore RL, Connolly M, et al. Definition and recommendations for advance care planning: an international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017;18(9):e543-e551.
[8] Quill TE, Abernethy AP. Palliative care–a burgeoning specialty. JAMA. 2013;310(10):1003-1004.
[9] Meier DE, Morrison RS. Palliative care transformation. JAMA. 2013;310(10):1005-1006.
[10] Brinkman-Stoppelenburg R, Rietjens JA, van der Heide A. The effects of advance care planning on end-of-life care: a systematic review. Palliat Med. 2014;28(8):1000-1025.
[11] Detering KM, Hancock HC, Reade MC, et al. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
[12] Bischoff KE, Sudore R, Miao Y, Boscardin WJ, Smith AK. Advance care planning and the quality of end-of-life care for older adults. J Am Geriatr Soc. 2013;61(3):337-344.
[13] Detering KM, Sellars M, Sinclair C, et al. Factors associated with completion of advance directives in older people: a population-based study. Age Ageing. 2009;38(5):541-546.
[14] Centers for Medicare & Medicaid Services. Medicare Learning Network. Advance Care Planning. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/AdvanceCarePlanning.pdf. Published January 2016. Accessed November 15, 2017.
[15] Hickman SE, Nelson CA, Perrin NA, Moss AH, Hammes BJ. POLST registry do-not-resuscitate orders and the outcomes of hospitalized patients. J Am Geriatr Soc. 2010;58(12):2281-2287.
[16] Wright AA, Zhang B, Ray A, et al. Associations between palliative chemotherapy and end-of-life care in women with metastatic breast cancer. J Clin Oncol. 2008;26(34):5570-5577.
[17] Earle CC, Park ER, Baker MD, et al. Barriers to the receipt of end-of-life cancer care as perceived by patients and their caregivers. J Clin Oncol. 2008;26(34):5578-5583.
[18] Barnato AE, Kozikowski C, Skinner J, et al. Is geographic variation in end-of-life care intensity explained by patient preferences? Med Care. 2007;45(3):192-199.
[19] Campbell ML, Guzman JA. Impact of palliative care consultation on hospital costs. Palliat Med. 2003;17(2):131-135.
[20] Gysels M, Higginson IJ. Is palliative care cost-effective? Curr Opin Support Palliat Care. 2008;2(1):1-5.
[21] Higginson IJ, Rumley J, material H, et al. Is there evidence that palliative care teams alter hospital use at the end of life? Palliat Med. 2004;18(5):375-386.
[22] Rabow MW, Dibble SL, Pantilat SZ, McPhee SJ. The comprehensive care team: a controlled trial of outpatient palliative medicine consultation. Arch Intern Med. 2004;164(1):83-91.
[23] Chen H, Morrison RS, Penrod J, et al.дено Cost and utilization outcomes of palliative care for patients with advanced cancer in a home-based primary care setting. J Pain Symptom Manage. 2008;36(6):581-588.
[24] Hughes SL, Weaver FM, Giobbie-Hurder A, et al. Effectiveness of team-based home care for frail older people: a randomized clinical trial. J Am Geriatr Soc. 2000;48(12):1625-1633.
[25] Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
[26] Kelley AS, Deb P, Du Q, Aldridge MD. Medicare expenditures in association with hospice enrollment and length of stay. Ann Intern Med. 2013;159(10):647-653.
[27] Connor SR, Pyenson B, Fitch K, et al. Comparing hospice and nonhospice care for patients who die within a year of a cancer diagnosis. J Pain Symptom Manage. 2007;33(3):238-246.
[28] Brumley R, Enguidanos E, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc. 2007;55(7):993-1000.
[29] Morrison RS, Maroney-Gifford CA, Zayas B, et al. Referral of patients with heart failure and cancer to palliative care: a systematic review. J Pain Symptom Manage. 2005;30(2):175-187.
[30] Centers for Medicare & Medicaid Services. Accountable Care Organizations (ACOs). https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ACO/. Published 2017. Accessed November 15, 2017.
[31] Sudore RL, Stewart AL, Knight SJ, et al. Development and validation of a questionnaire to assess advance care planning. J Palliat Med. 2009;12(7):617-626.
[32] Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619.
[33] Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 7th ed. New York: Oxford University Press; 2013.
[34] United States Conference of Catholic Bishops. Ethical and Religious Directives for Catholic Health Care Services. 6th ed. Washington, DC: US Conference of Catholic Bishops; 2016.
[35] Molloy DW, Guyatt GH, Russo R, et al. Systematic implementation of an advance directive program in nursing homes: a randomized controlled trial. JAMA. 2000;284(11):1437-1444.
[36] Engelhardt JB, McClatchey MW, Madan A, et al. Impact of care coordination on costs and utilization of health care services: a randomized controlled trial in a high-risk population. Am J Manag Care. 2013;19(5):e165-e174.
[37] SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT). JAMA. 1995;274(20):1591-1598.
[38] Hamlet J, Panzer R, Johnson N, et al. The cost-effectiveness of palliative care: a secondary analysis of the SUPPORT study. J Pain Symptom Manage. 2006;32(1):1-12.
[39] Bernacki RE, Block SD; American Academy of Hospice and Palliative Medicine Ethics Committee. American Academy of Hospice and Palliative Medicine Ethics Committee. Communication about prognosis and advance care planning. Ann Intern Med. 2014;161(1):73-80.
[40] Weeks JC, Catalano PJ, Cronin AM, et al. Patients’ expectations about effects of chemotherapy for advanced cancer. J Clin Oncol. 2012;30(12):1293-1299.
[41] Centers for Medicare & Medicaid Services. Fast Facts. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/CMS-Fast-Facts/index.html. Published 2017. Accessed November 15, 2017.
[42] Xu JQ, Murphy SL, Kochanek KD, Bastian BA. Deaths: Final Data for 2013. National Vital Statistics Reports. 2016;64(2).