
Effective Diabetes Care Management Programs are crucial for improving patient outcomes and reducing the burden of this chronic disease. Despite established guidelines for diabetes care, many adults still struggle to achieve optimal glycemic control. This meta-analysis examines the effectiveness of diabetes care management programs in improving glycemic control, measured by glycated hemoglobin (HbA1c) levels, and identifies the key components that contribute to program success.
Methods
This study rigorously analyzed randomized controlled trials (RCTs) to evaluate the impact of diabetes care management programs.
Defining Diabetes Care Management Programs
For this meta-analysis, diabetes care management was defined as ongoing, proactive patient follow-up incorporating at least two of the following elements:
- Patient Education: Covering diet and exercise counseling, self-monitoring techniques, and comprehensive disease and medication knowledge.
- Coaching: Providing encouragement and support to patients to overcome psychological or social barriers hindering self-management and medication adherence.
- Treatment Adjustment: Enabling disease managers to initiate or modify treatment plans, with or without prior approval from a primary care physician.
- Monitoring: Regular collection of patient medical data by the disease manager to track progress and identify potential issues.
- Care Coordination: Proactive measures such as appointment reminders, reinforcement of self-care strategies, and communication of patient status, complications, and treatment recommendations to primary care physicians.
Literature Search Strategy
A comprehensive literature search was conducted across MEDLINE, Scopus, Web of Science, and the Cochrane Library, encompassing publications up to December 2009. The search strategy employed keywords such as “patient care team,” “disease management,” “case management,” “managed care programs,” “home-based intervention,” and “patient care management,” alongside terms specific to diabetes and glycemic control, including “diabetes mellitus,” “HbA1C,” and “glycated hemoglobin.” Reference lists of identified studies were also manually searched to ensure maximal capture of relevant trials.
Selection criteria mandated that studies were RCTs involving adults with type 1 or type 2 diabetes, evaluating the effect of disease-management programs on HbA1c concentrations. Studies had to report HbA1c levels both before and after the intervention, with post-intervention assessment occurring at least 12 weeks after program initiation. Studies were excluded if the intervention lacked direct contact between the disease manager and the patient, or if contact was exclusively via internet or mail.
Data Extraction and Statistical Analysis
Two independent reviewers meticulously extracted data from each included study. Extracted data included patient demographics, sample size, intervention characteristics (components, duration, frequency of contact, mode of delivery), HbA1c levels at baseline and post-intervention, and reported adverse events. Contact frequency was categorized as low (less than monthly), moderate (monthly), or high (more than monthly). Discrepancies in data extraction and frequency classification were resolved through consensus and review by a third reviewer.
Statistical analysis employed a random-effects model to calculate the pooled standardized mean difference in HbA1c levels between intervention and control groups, accounting for baseline HbA1c variations across studies. Meta-regression analysis was utilized to explore the association between program components and patient characteristics with HbA1c outcomes. Sensitivity analyses were performed to assess the robustness of findings based on study quality indicators such as dropout rates and allocation concealment.
Results
Study Characteristics
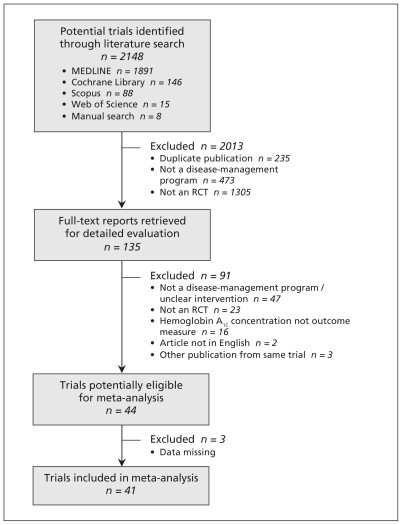
The systematic search and selection process, outlined in Figure 1, identified 41 RCTs for inclusion in the meta-analysis. These trials, published between 1990 and 2009, involved 7013 adults with type 1 or type 2 diabetes.
The characteristics of the included RCTs are detailed in Table 1. The majority of trials focused on type 2 diabetes, with interventions ranging from 1.5 to 48 months in duration. Intervention modes included face-to-face sessions, phone contact, or a combination of both.
Impact on Glycemic Control
Diabetes care management programs demonstrated a statistically significant and clinically relevant improvement in glycemic control. The pooled standardized mean difference in HbA1c levels between intervention and control groups was -0.38 (95% CI -0.47 to -0.29, p<0.001). This corresponds to an absolute mean reduction of 0.51% in HbA1c levels, favoring diabetes management programs over usual care. Figure 2 visually represents the estimated differences in HbA1c levels.
Key Components of Effective Programs
Meta-regression analysis identified specific components of diabetes care management programs associated with greater HbA1c reduction. Programs that empowered disease managers to adjust treatment regimens, with or without physician pre-approval, showed significantly greater improvement in HbA1c levels (standardized mean difference -0.60 vs -0.28, p=0.004).
Furthermore, the frequency of patient contact emerged as a critical factor. Programs with high contact frequency demonstrated a significantly larger reduction in HbA1c compared to programs with low contact frequency (standardized mean difference -0.56 vs -0.30, p=0.03). While programs with moderate or high contact frequency showed significant HbA1c reduction compared to usual care, only high-frequency contact programs were significantly more effective than low-frequency contact programs.
Patient education mode (individual vs. group), intervention mode (phone, face-to-face, or combined), intervention length, and feedback of initial evaluation to the primary care physician did not significantly modify program effectiveness in subgroup analyses. However, treatment adjustment and patient education mode accounted for a substantial portion of the variance between trials.
Sensitivity Analyses
Sensitivity analyses, based on dropout rates and allocation concealment, confirmed the robustness of the primary findings, indicating that the observed effectiveness of diabetes care management programs was not significantly influenced by study quality variations.
Adverse Events
Hypoglycemic episodes were not systematically reported across studies. Among the studies that did report hypoglycemia, no consistent difference was observed between intervention and control groups. Mortality rates were also similar between groups. Hospital admissions were not consistently reported.
Interpretation
This meta-analysis provides compelling evidence for the clinical effectiveness of diabetes care management programs in improving glycemic control in adults with diabetes. The observed 0.51% absolute reduction in HbA1c is clinically meaningful, as even a 1% reduction in HbA1c is associated with significant reductions in diabetes-related complications.
The study highlights two key components for successful diabetes care management programs: treatment adjustment by disease managers and high frequency of patient contact.
Treatment Adjustment: Allowing disease managers to proactively adjust medication regimens, whether independently or in collaboration with physicians, appears crucial. This proactive approach can address treatment non-adherence, a major barrier to glycemic control.
Frequency of Contact: Intensive, high-frequency contact between disease managers and patients is more effective. This suggests that sustained engagement and support are essential for behavior change and improved self-management. Programs with less intensive contact may not yield the same level of benefit.
While patient education is a cornerstone of diabetes care, the mode of delivery (individual vs. group) did not significantly impact outcomes in this analysis. This suggests that both individual and combined group/individual education strategies can be effective components of diabetes management programs.
The finding that programs are more effective in patients with poorer baseline glycemic control (HbA1c ≥ 8.0%) suggests that diabetes management programs may be particularly beneficial for individuals with uncontrolled diabetes who are at higher risk for complications.
Strengths and Limitations
The strengths of this meta-analysis include its comprehensive literature search, inclusion of a large number of RCTs, and robust statistical methodology. The findings are consistent with previous reviews, but this study provides a more precise estimate of effectiveness due to the inclusion of more recent trials and a larger sample size.
Limitations include the restriction to English-language publications, potential for missing unpublished studies, and heterogeneity across trials. The analysis relied on study-level data, and the limited reporting of intervention details in some studies precluded a more granular analysis of all potentially relevant program components. The relatively short follow-up duration in many trials limits conclusions about long-term impacts on diabetes complications.
Conclusion
Diabetes care management programs are a valuable strategy for improving glycemic control in adults with diabetes. For optimal effectiveness, programs should incorporate high-frequency patient contact and empower disease managers to adjust treatment plans. Prioritizing intensive, proactive programs targeting high-risk patients with poorly controlled diabetes may yield the greatest clinical benefit.
Further research is needed to evaluate the long-term impact of diabetes care management programs on diabetes complications, healthcare utilization, and cost-effectiveness. Identifying specific patient subgroups that benefit most from different program components is also an important area for future investigation.
Note: Tables and Supplementary Materials from the original article are not included here as per instructions to only include title and content. References are also omitted to maintain focus on content generation as per the prompt. If references are needed, they can be easily extracted from the original article.