
Asthma remains a prevalent chronic disease among children, particularly affecting minority and low-income communities. Understanding effective interventions is crucial to address health disparities and improve outcomes for vulnerable populations. This article delves into a significant randomized clinical trial that investigated the effectiveness of a comprehensive asthma educational program for preschool children enrolled in Head Start. The study compared a multilevel intervention, integrating both home and school-based education, against a school-based program alone. The findings offer valuable insights into strategies for enhancing asthma care and reducing health inequities in young children.
The Critical Need for Improved Asthma Care Programs
Asthma is the most common chronic childhood illness, and its burden is not evenly distributed. Alarmingly, Black children experience disproportionately higher rates of morbidity and mortality from asthma. Preschool-aged children, in particular, face the greatest risk of healthcare service utilization due to asthma. These early health disparities can have long-lasting consequences, highlighting the urgent need for effective interventions that begin early in life.
Addressing asthma disparities requires innovative and multifaceted strategies tailored to the unique challenges faced by low-income and minority families. While advancements in asthma therapies and clinical guidelines are available, their impact has not been uniform across all populations. Effective asthma educational programs are essential to bridge this gap and empower families and communities to better manage this condition.
Previous research has demonstrated the potential of asthma education programs in improving asthma management for preschool children. One such program, Asthma Basic Care (ABC), has shown promise in reducing symptoms and oral corticosteroid use in emergency department settings. However, broader implementation and evaluation of such programs in community settings are necessary to achieve a wider public health impact, making programs like an “Eakin Care Program” in a general sense highly relevant.
Head Start: A Vital Community Partner for Asthma Intervention
For asthma interventions to be truly effective and sustainable for vulnerable children, they must be integrated into community structures that serve these high-risk populations. Head Start, a federally funded national program, emerges as an ideal partner. By providing preventive health services and engaging parents, Head Start offers a crucial platform for disseminating asthma education early in a child’s life. In Maryland, Head Start stands as one of the largest childcare providers for low-income families, making it a strategic setting for widespread implementation of asthma programs.
This study evaluated the effectiveness of integrating the evidence-based Asthma Basic Care (ABC) family educational program within the existing Head Start asthma education framework. The central hypothesis was that children receiving the combined ABC plus Head Start program would experience a greater reduction in asthma morbidity compared to those receiving Head Start education alone. The primary outcome measured was the improvement in asthma control, assessed using the Test of Respiratory and Asthma Control in Kids (TRACK) score. Secondary outcomes included healthcare utilization, oral corticosteroid courses, and caregiver quality of life related to asthma management.
Study Design and Methodology
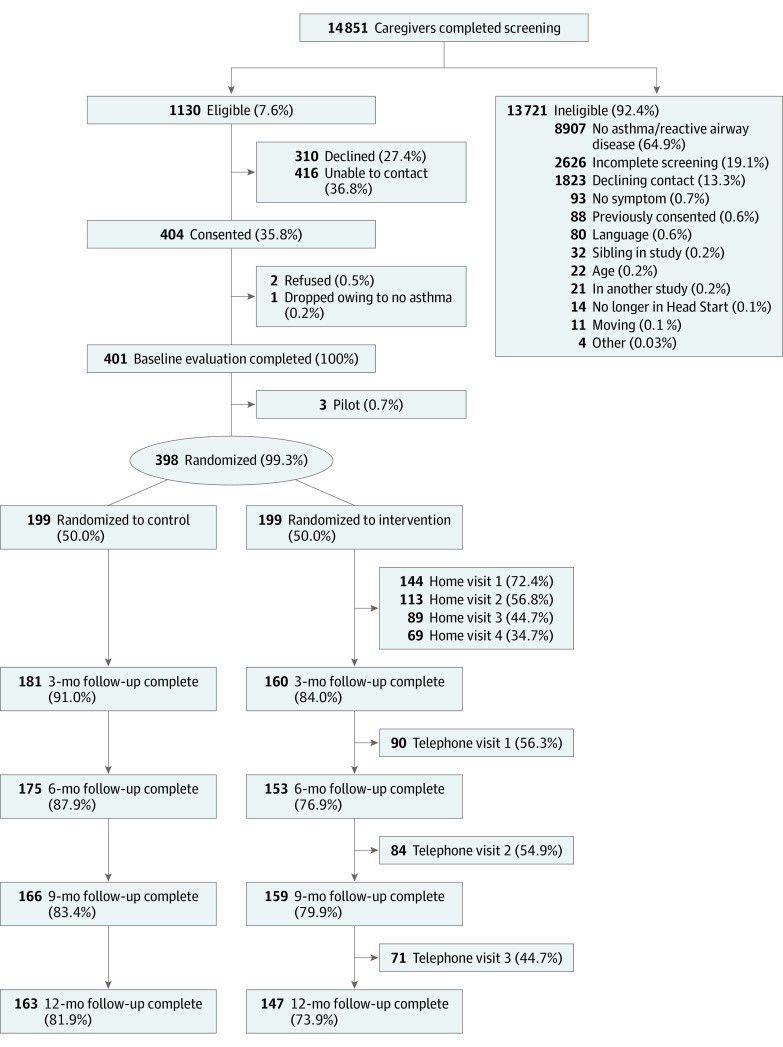
This randomized clinical trial was conducted across 14 Head Start programs in Baltimore, Maryland, involving 398 preschool children with asthma and their primary caregivers. Participants were recruited between 2011 and 2016, with data collection concluding in 2017. The study protocol received approval from the Johns Hopkins School of Medicine Institutional Review Board, and informed consent was obtained from all caregivers.
Participants and Recruitment
Children aged 2 to 6 years with a physician-diagnosed asthma and English-speaking caregivers were eligible for participation. Physician diagnosis was verified with the child’s primary care provider. Recruitment involved biannual screenings of Head Start students using a questionnaire administered by Head Start staff. Families expressing interest were contacted to confirm eligibility and schedule home visits.
Randomization and Blinding
Eligible families were randomly assigned in a 1:1 ratio to either the ABC plus Head Start education group or the Head Start education alone group. Randomization was stratified in blocks of 10 to ensure balanced group sizes. While families were not blinded to their assigned group, research assistants conducting assessments were blinded and were separate from intervention staff.
Intervention Programs
Head Start Asthma Education (Control Group): All participating Head Start programs implemented a comprehensive asthma education program. This included annual asthma training for Head Start staff, conducted by the research team. Training covered asthma symptom management, medication use, trigger identification, and communication with families. Expert facilitators provided ongoing guidance to each Head Start program, supporting asthma awareness activities such as parent workshops and health fairs.
Asthma Basic Care (ABC) plus Head Start Education (Intervention Group): In addition to the Head Start program, this group received the Asthma Basic Care (ABC) family intervention. ABC consisted of four in-person, at-home educational sessions (30-45 minutes each) and three follow-up booster calls. Interventionists, including Head Start staff and Johns Hopkins asthma educators, delivered tailored education using iPads with visual and video content suitable for low health literacy. Content was based on national guidelines and addressed key asthma management areas, including medication, action plans, trigger avoidance, and symptom management. Families engaged in problem-solving and goal-setting with interventionists.
Data Collection and Measures
Data were collected at baseline, 3, 6, 9, and 12 months through home and telephone visits conducted by research assistants.
- Primary Outcome: Asthma control was measured using the Test for Respiratory and Asthma Control in Kids (TRACK) score, a validated tool for preschool children. Higher scores indicate better asthma control.
- Secondary Outcomes:
- Healthcare utilization (emergency department visits, hospitalizations) and oral corticosteroid courses were reported by caregivers.
- Caregiver health-related quality of life was assessed using the Pediatric Asthma Caregiver’s Quality of Life Questionnaire (PACQLQ).
Statistical Analysis
Generalized estimating equations were used to compare outcomes between groups over time, controlling for baseline levels and seasonal variations. Logistic regression was used to analyze hospitalization data due to its low frequency. Intention-to-treat analyses were performed, and sensitivity analyses were conducted to assess the robustness of the findings.
Key Findings and Outcomes
Improved Asthma Control with Multilevel Intervention
The study revealed a significant overall improvement in asthma control for both groups over the 12-month period. However, the ABC plus Head Start group demonstrated a greater improvement in asthma control scores compared to the Head Start alone group, particularly at the 12-month mark. Furthermore, at 3 months, a significantly smaller proportion of children in the ABC plus Head Start group had uncontrolled asthma.
TRACK Score Improvements: The ABC plus Head Start program led to a more pronounced and sustained improvement in TRACK scores, indicating better asthma management in this group.
Reduced Uncontrolled Asthma: Children receiving the combined intervention were less likely to have uncontrolled asthma, especially in the initial months following the intervention.
Reduction in Healthcare Utilization
A key benefit of the multilevel intervention was a significant reduction in hospitalizations. Children in the ABC plus Head Start group were significantly less likely to be hospitalized for asthma during the 12-month follow-up period compared to the Head Start alone group. Additionally, at 9 months, the ABC plus Head Start group showed a significant reduction in courses of oral corticosteroids.
Fewer Hospitalizations: The combined program effectively reduced the need for hospital care, a critical outcome for children with asthma and their families.
Reduced Oral Corticosteroid Use: The intervention also contributed to a decrease in the use of oral corticosteroids, medications often used to manage severe asthma exacerbations.
Enhanced Quality of Life
Both groups experienced improvements in asthma-related quality of life for caregivers over the 12 months. This indicates that both educational programs had a positive impact on families’ ability to manage their children’s asthma and its effects on their lives.
Discussion and Implications
This study provides compelling evidence for the effectiveness of a multilevel asthma intervention, integrating home-based family education (ABC) with a school-based Head Start program, in improving asthma outcomes for low-income minority preschool children. The combined program demonstrated a modest but significant effect on asthma control, reduced hospitalizations, and decreased oral corticosteroid use compared to school-based education alone.
Multilevel Approach for Vulnerable Populations
The success of the ABC plus Head Start program underscores the importance of multilevel interventions in addressing health disparities. By targeting both the home and school environments, the program effectively reinforced asthma management strategies and provided comprehensive support for families. This approach is particularly crucial for preschool children who spend significant time in both settings.
Community-Based Partnerships
The study highlights the value of partnering with community organizations like Head Start. Leveraging Head Start’s existing infrastructure and trusted relationships with families facilitated the effective implementation and reach of the asthma intervention. Such community-based partnerships are essential for sustainable public health impact, especially in reaching vulnerable populations.
Innovation in Education Delivery
The use of technology, specifically iPads, to deliver guideline-based asthma education during home visits was a novel aspect of this intervention. This approach allowed for tailored education, incorporation of visual aids, and enhanced engagement, particularly for families with low health literacy.
Addressing Health Disparities
This research contributes significantly to addressing health disparities in pediatric asthma. By demonstrating the effectiveness of a culturally sensitive and community-integrated intervention in a high-risk population, the study offers a promising model for reducing asthma inequities. The findings suggest that focusing on multilevel interventions within community settings can be a key strategy in mitigating disparities and improving outcomes for vulnerable children.
Limitations
It is important to acknowledge certain limitations of this study. The primary outcome was changed from symptom-free days to asthma control based on recommendations from the data safety monitoring board. Healthcare utilization data relied on caregiver reports, which may be subject to recall bias, although previous research suggests reasonable accuracy in caregiver recall of urgent healthcare use. The study population was primarily low-income and African American, which may limit generalizability to other populations, but also represents a strength in identifying effective interventions for a high-risk group. Selection bias may have occurred due to the voluntary nature of participation and the requirement for home and telephone visits.
Conclusion and Future Directions
This randomized clinical trial provides strong evidence for the benefits of combining a home-based family education program (ABC) with a Head Start educational program to improve asthma control and reduce healthcare utilization in preschool children. The multilevel intervention approach, delivered in partnership with a community organization like Head Start, holds significant promise for addressing asthma disparities and enhancing the health of vulnerable populations.
Future research should focus on evaluating the cost-effectiveness of this intervention and exploring strategies for broader implementation through partnerships with community organizations and policy development. Further investigation into the long-term sustainability of these positive outcomes and the optimal components of multilevel asthma care programs is also warranted. By continuing to innovate and implement evidence-based programs like this, we can make significant strides in improving the lives of children with asthma, especially those in underserved communities, ensuring they receive the comprehensive care, perhaps through programs like an “eakin care program” in principle, they need to thrive.