
Introduction
The period immediately following hospital discharge is fraught with challenges for patients, with approximately one in five experiencing adverse events, including adverse drug events (ADEs) and hospital-related complications.1–3 Alarmingly, hospital readmission rates remain high, with nearly 20% of older Medicare patients readmitted within 30 days.1 This critical juncture underscores the urgent need for effective Transition Care Programs to ensure patient safety and well-being beyond the hospital walls.
Post-discharge adverse events encompass a wide range of issues, from diagnostic and therapeutic errors to infections, but ADEs stand out as particularly prevalent and harmful, frequently leading to further hospitalizations and readmissions.4,5 Studies reveal that nearly 100,000 elderly patients are hospitalized annually due to ADEs.6 Patients with neurological conditions, such as stroke, face an elevated risk of recurrent cerebrovascular events, repeated hospitalizations within a year, increased disability, and higher mortality rates.7,8 Therefore, establishing robust transition care programs is paramount for neurohospitalists to safeguard patients with complex, chronic neurological illnesses like stroke, demyelinating diseases, epilepsy, and neuromuscular conditions.9
Transition care, fundamentally, is the comprehensive support patients receive as they navigate between different healthcare settings and providers. It is about effectively bridging gaps in care during transitions, whether from hospital to home or between inpatient and outpatient services.10,11 Hospital-based transition care interventions are designed to facilitate a seamless shift from the inpatient to the outpatient environment, proactively preventing avoidable readmissions and adverse events.
Recognizing the significant financial implications of adverse events and readmissions, several national policy initiatives have been implemented to drive improvements in transition care. The Centers for Medicare & Medicaid Services (CMS) already publicly reports hospitals’ risk-adjusted 30-day readmission rates for key conditions like pneumonia, acute myocardial infarction, and congestive heart failure (CHF).12 Anticipating future expansion, it is expected that other diagnoses, including neurological conditions such as stroke, may be included in these public reporting metrics.13 CMS has already imposed financial penalties on over 2,000 hospitals with high readmission rates, potentially reaching up to 1% of Medicare reimbursements.14 Furthermore, the Partnership for Patients initiative aimed to reduce preventable readmissions by 20% by the end of 2013, highlighting improved transition care as a crucial strategy to lower healthcare expenditures.15 These policies collectively mandate hospitals to prioritize and enhance transition care for patients upon hospital discharge.
While disease-specific transition care programs have shown some success in reducing readmissions for conditions like CHF, chronic obstructive pulmonary disease, and asthma, effective strategies for neurological diseases remain less defined. Systematic reviews have identified various studied interventions,16–19 but their impact on readmissions and other critical post-discharge patient safety indicators, such as emergency department (ED) visits and adverse events, is not well-established.
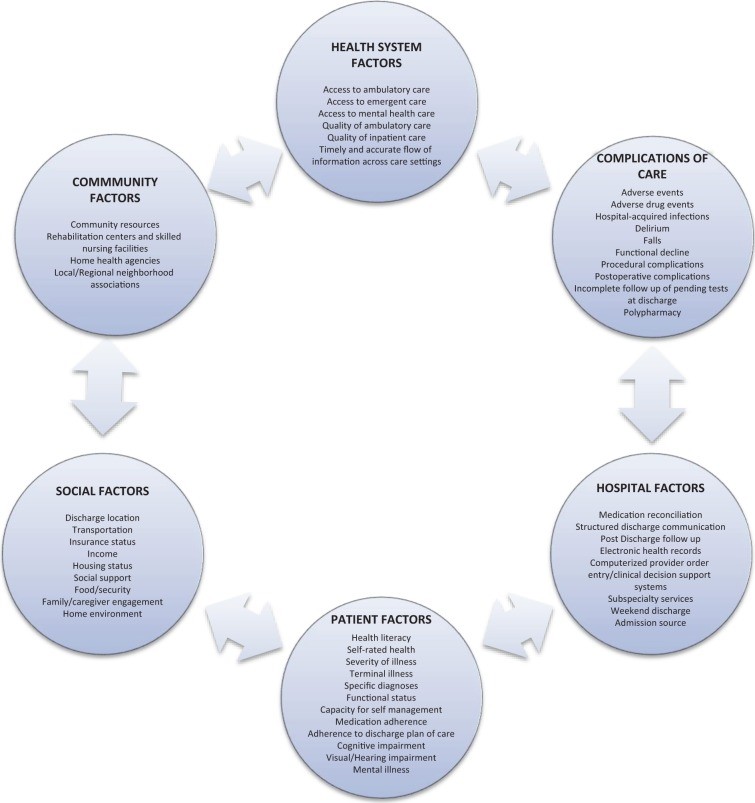
Data suggests that nearly 20% of 30-day readmissions are preventable, based on readmission risk factor studies.20 Hospital readmission rates are significantly influenced by factors outside the hospital setting, including inadequate social support, poverty, and limited access to outpatient care (Figure 1).21–23 A retrospective review of stroke and cerebrovascular disease discharges from a single academic medical center revealed that 53% of readmissions were potentially avoidable, often due to gaps in care coordination, delayed follow-up, and insufficient discharge instructions.24 Despite these complexities, progress is evident, with CMS reporting a decline in 30-day readmission rates for Medicare patients between 2007 and 2012.25
Figure 1.
 Factors involved in hospital readmission
Factors involved in hospital readmission
In an era focused on high-value, cost-effective healthcare solutions, transition care programs demand strategic resource allocation, particularly human resources, to maximize their effectiveness. These programs align with the core values of neurohospitalists and patients by prioritizing improved care quality, enhanced patient safety, and seamless healthcare system connectivity. This review will delve into the characteristics of effective transition care strategies, evaluate the efficacy of several established programs, and offer specific recommendations for neurohospitalists to implement impactful transition care programs.
Defining Transition Care: Strategies, Risks, and Adverse Events
Classifying Strategies and Adverse Events
A transition care strategy encompasses any intervention or set of interventions initiated before hospital discharge, explicitly aimed at facilitating a safe and effective patient transition from one care setting to another, such as hospital to home. These interventions are broadly categorized into three types: predischarge, postdischarge, and “bridging” interventions, which incorporate both pre- and postdischarge components (Table 1).17,26–30
Table 1.
Taxonomy of Interventions to Improve Transition Care at Hospital Discharge.
| Predischarge interventions | Assessment of risk of adverse events or readmissions |
|---|---|
| Patient engagement (e.g., patient or caregiver education) | |
| Creation of an individualized patient record (customized document in lay language containing clinical and educational information for patients’ use after discharge) | |
| Facilitation of communication with outpatient providers | |
| Multidisciplinary discharge planning team | |
| Dedicated transition provider (who has in-person or phone contact with the patient before and after discharge) | |
| Medication reconciliation | |
| Postdischarge interventions | Outreach to patients (including follow-up phone calls, patient-activated hotlines, and home visits) |
| Facilitation of clinical follow-up (including facilitated ambulatory provider follow-up) | |
| Medication reconciliation after discharge | |
| Bridging interventions | Inclusion of at least 1 predischarge component and at least 1 postdischarge component |
Post-discharge adverse events are defined as clinically significant injuries occurring after hospital discharge, encompassing new or worsening symptoms, abnormal lab results requiring clinical management changes, and injuries (such as ADEs, falls, or hospital-acquired infections) partly or wholly attributable to hospital care. This definition aligns with classifications used in prior epidemiological studies of post-discharge adverse events.3,4 In research, readmission is often considered an adverse event and is measured at various intervals: 30-day, 60-day, 90-day, and 6-month readmission rates from the initial hospitalization.
Identifying Readmission and Adverse Event Risks
Predicting precisely which patients will be readmitted or experience adverse events remains challenging. However, certain patient groups are demonstrably at higher risk in the post-hospitalization period. These include older adults, individuals with chronic illnesses, and those hospitalized for stroke, primarily due to fragmented care, transitions across multiple care settings, and frequent provider handoffs.1,3,17,31–33 Studies have identified several risk factors for hospital readmission and poorer outcomes in neurological patients, such as poor functional status at discharge, advanced age, psychiatric illness, and limited social support services.34–36 A systematic review assessing predictors of readmission after stroke found no standardized risk-prediction models that could reliably compare or predict readmissions across different hospitals.37
Despite the absence of standardized prediction tools, older adults and individuals with multiple chronic conditions constitute a significant portion of admissions and readmissions to inpatient neurology services. Stroke patients are frequently readmitted for cerebrovascular, cardiac, and non-cardiac issues, including urinary tract infections, pneumonia, and hip fractures.8,38,39
Exemplary Transition Care Strategies
The following four transition care programs are highlighted based on evidence from multiple controlled trials demonstrating their effectiveness in reducing readmissions (Table 2).
Table 2.
Highlighted Hospital-Based Transition Care Programs.
| Programs | Strategies | Description/Effectiveness |
|---|---|---|
| Care Transitions Intervention40–43 | Patient engagement Individualized patient record Dedicated transition provider Facilitation of communication to outpatient providers Outreach Medication reconciliation | Focuses on 4 domains of care including self management skills. Studied in several settings. CCT40,43 and RCT41,42. Decreased 30-day readmission rates: ARR 4.9%,40 ARR 3.6%,41 and ARR 5.8%43. Decreased 90-day readmission rates: ARR 5.8%41 and ARR 21.7%42. 30-Day ED visits: ARR 3.2% (NS)40 |
| Transitional Care Model44–47 | Patient engagement Individualized patient record Dedicated transition provider Facilitation of communication to outpatient providers Facilitated clinical follow-up Outreach | Nurse-led program studied in geriatric patients, intensive outreach with home and telephone follow-up. RCT. Decreased 90-day readmission rates: ARR 16.8%44 (within 24 weeks), ARR 48.0%,45 and ARR 13%46 (within 6 weeks). ED visits (within 24 week): NS44,47. Adverse events (postdischarge infection) ARR 16.7% (NS)45 |
| Project RED48 | Patient engagement Individualized patient record Dedicated transition provider Facilitation of communication to outpatient provider Multidisciplinary team Outreach Medication reconciliation (predischarge and postdischarge) | Team-based program included pharmacist outreach and medication reconciliation. RCT. Decreased 30-day readmission rates: ARR 5.8% (NS). Decreased 30-day ED visits: ARR 8.0% |
| Project BOOST49–52 | Patient engagement Multidisciplinary team Outreach Medication reconciliation Risk assessment | Multicenter QI program with mentored implementation. CCT49 and pre–post study51. Decreased 30-day readmission rates: ARR 2%51 and ARR 5.9%49 |
Abbreviations: ARR, absolute risk reduction; CCT, clinical controlled trial (nonrandomized); ED, emergency department; NS, not significant; QI, quality improvement; RCT, randomized controlled trial; RED, Reengineered Discharge; BOOST, Better Outcomes for Older Adults Through Safe Transitions.
Care Transitions Intervention
The Care Transitions Intervention (CTI), pioneered by Eric Coleman at the University of Colorado, is a multifaceted transition care program widely adopted across numerous hospitals.40–43 Studies have included older adults admitted for stroke and various chronic illnesses. CTI’s primary goals are to actively engage patients and empower them and their caregivers in self-management post-hospitalization, equipping them with the skills to effectively navigate the healthcare system. The intervention is structured around four core pillars: (1) medication management, (2) development of a personal health record for seamless information transfer across care settings, (3) ensured follow-up with a primary care provider, and (4) identification of “red flags” signaling the need to contact healthcare providers. A dedicated “transition coach,” typically an advanced practice nurse, conducts post-discharge home visits and telephone calls, reinforcing patient engagement and self-management of chronic conditions. Evaluations across diverse acute care settings, including managed care, capitated delivery systems, and Medicare fee-for-service populations, have demonstrated statistically significant reductions in 30-day readmission rates attributed to this transition care program.
The Transitional Care Model
The Transitional Care Model (TCM), another nationally recognized transition care program developed by Mary Naylor at the University of Pennsylvania, focuses on hospital-based discharge planning and home follow-up for high-risk, chronically ill older adults. It has been specifically studied in older adults with CHF and myocardial infarction.44–47 While specific neurological diagnoses were not detailed in published studies, the model’s principles are broadly applicable. A transitional care nurse (TCN) provides continuous support to patients from hospital to home, facilitating communication between inpatient and outpatient providers, and conducting a series of home visits and follow-up phone calls post-discharge. TCM emphasizes a multidisciplinary approach to patient care, with the TCN acting as a central coordinator, maintaining contact with physicians, nurses, social workers, discharge planners, and pharmacists. Multiple studies have shown significant reductions in readmission rates at both 60 and 90 days with this comprehensive transition care program.
Project RED
Project Reengineered Discharge (RED) is a transition care program implemented in a general medicine population within an urban safety net hospital. It emphasizes a multidisciplinary approach to patient care, coordinated by a nurse discharge advocate (DA).48 The DA actively engages patients during their hospitalization, providing crucial clinical information and a personalized, illustrated post-hospitalization plan. Following discharge, a pharmacist conducts telephone follow-ups, including a thorough medication review and direct communication with the patient’s primary outpatient provider. The initial Project RED study, while not specifying neurological diagnoses among enrolled patients, demonstrated significant reductions in hospital utilization, defined as combined ED visits and readmissions, within 30 days of discharge, approximately 30% lower in the intervention group. This highlights the potential of a well-structured transition care program to improve outcomes across various patient populations.
Project BOOST
Project Better Outcomes for Older Adults Through Safe Transitions (BOOST) is a transition care program supported by the Society of Hospital Medicine.49–52 This quality improvement collaborative has been implemented in diverse hospital settings across the United States, targeting general medicine and medical-surgical patient populations. Mentors, who are hospitalist experts in quality improvement and care transitions, guide the development and implementation of BOOST programs tailored to each hospital’s specific needs. The BOOST toolkit includes various interventions such as risk assessment, medication reconciliation, discharge checklists, and a multidisciplinary team-based approach to the discharge process. A recent study across 30 hospitals demonstrated modest reductions in readmission rates, although data was only available from 11 participating hospitals.51 This underscores the value of collaborative, mentored approaches in implementing effective transition care programs.
Strategies Tailored for Neurologic Patients
Several studies have specifically evaluated the effectiveness of transition care programs for stroke patients. A systematic review of 27 such studies concluded that a limited number provided low-to-moderate evidence that hospital-initiated interventions improved certain outcomes, such as reduced hospital days and improved physical activity. However, these studies did not consistently demonstrate an impact on readmissions or mortality.34 Despite the limited evidence of reduced healthcare utilization or adverse events, the review authors emphasized that hospital-initiated strategies focused on care coordination remain crucial for improving healthcare quality in this vulnerable patient population. Specific interventions, such as secondary stroke prevention measures (antithrombotic, antihypertensive, and lipid-lowering agents), dysphagia screening, and reducing unnecessary urinary catheter use during hospitalization, have been shown in published studies to decrease readmissions and post-discharge adverse events like cerebrovascular accidents, pneumonia, and catheter-associated urinary tract infections.53–59 Neurohospitalists are uniquely positioned to directly influence patient care beyond the hospital stay by implementing interventions that enhance care quality, reduce costs, and mitigate the risks associated with preventable readmissions and adverse events through targeted transition care programs.
Key Elements of Successful Transition Care Programs
These exemplary transition care programs share several common characteristics. Notably, both general programs and many stroke-specific programs incorporate bridging interventions, utilizing a dedicated transition provider, often a nurse or case manager, as the clinical lead. A consistent emphasis is placed on having a patient advocate who facilitates care coordination and proactively reaches out to patients post-hospitalization. Similar to general medicine populations, neurological patients benefit significantly from transition care strategies that prioritize improved communication across care settings, proactive patient outreach, and robust patient engagement.
Implementation Considerations and Program Costs
While descriptions of numerous transition care programs often include timelines and intervention details, information regarding program costs, resource requirements for implementation, and strategies for ensuring long-term sustainability is frequently lacking. This gap in knowledge represents a critical area for future research and program development.
Discussion
This review has provided a framework for understanding transition care strategies aimed at decreasing hospital readmissions and post-discharge adverse events, highlighting four nationally recognized and effective programs. A key finding is that nearly all successful transition care programs published over the past two decades incorporate bridging interventions and rely on a dedicated clinical lead, a transition provider who engages with patients both before and after hospital discharge. Three of these programs—CTI, Project BOOST, and TCM—have been successfully implemented and evaluated across diverse patient populations and healthcare systems. Project RED, another effective intervention, has been successfully deployed within a safety net system. While these strategies are resource-intensive, evidence strongly suggests their effectiveness in improving patient outcomes and reducing readmissions. However, further research is needed to address the current lack of detailed information on program implementation, long-term sustainability, and comprehensive cost analyses of various transition care programs. Specifically, more evidence is required to draw definitive conclusions about the impact of these specific strategies on patients with acute neurological illnesses.
Recommendations for Neurohospitalists
Hospitals and neurohospitalists are increasingly challenged to develop and implement effective transition care programs that demonstrably reduce readmissions and mitigate financial penalties. Current research strongly supports the use of multidisciplinary, multicomponent strategies incorporating bridging interventions and a dedicated transition clinician. Programs like CTI, TCM, Project RED, and Project BOOST have been rigorously studied and successfully replicated across the United States, providing valuable models for implementation. It is crucial to acknowledge that each hospital network possesses unique internal factors, organizational culture, community demographics, and geographical considerations that will influence the optimal transition care program design. A “one-size-fits-all” approach is unlikely to be effective in transition care. However, core elements of a successful transition care strategy consistently include: robust patient engagement, utilization of a dedicated transition provider, comprehensive medication management (including medication reconciliation), facilitated communication with outpatient providers, and proactive patient outreach (Table 3). Furthermore, disease-specific interventions tailored for the neurology patient population can be effectively integrated into a broader transition care program, such as home care protocols for disease monitoring, medication adherence support, symptom management guidelines, and direct communication pathways with rehabilitation programs.
Table 3.
Summary Recommendations for Neurohospitalists Implementing a Transition Care Program.
| Key Actions for Implementing a Transition Care Program |
|---|
| Obtain hospital-specific data on 30-day readmission rates (both all-cause and disease- or unit-specific rates) to understand baseline performance and areas for improvement. |
| Assess your hospital’s existing quality improvement and patient safety infrastructure, including electronic health record capabilities and prior experience with quality improvement initiatives, to leverage existing resources. |
| Create an interdisciplinary team and identify passionate champions within different departments to drive the implementation and ongoing success of the transition care program. |
| Define clear, measurable outcomes to track the program’s effectiveness, such as 30-day readmission rates, adverse drug events, and medication errors, allowing for data-driven program adjustments. |
| Implement a bundled (multicomponent) transition care strategy that incorporates patient engagement, a dedicated transitions provider, medication reconciliation, facilitated communication, and patient outreach to address multiple facets of care transition. |
| Incorporate disease-specific interventions relevant to the neurology patient population, such as secondary stroke prevention protocols and dysphagia screening, to tailor the program to specific patient needs. |
Neurohospitalists, in their roles as both primary providers and consultants, are uniquely positioned to provide crucial expertise and leadership in initiatives aimed at enhancing transition care for a diverse range of patients. For example, neurohospitalists can spearhead disease-specific initiatives like delirium and dysphagia screening for patients with cerebrovascular and neurological diseases. They can also effectively collaborate with medicine hospitalists on broader, institution-wide transition care strategies like those described previously.60–62 As consultants, neurohospitalists can offer evidence-based recommendations to reduce readmission risks and other adverse events, such as implementing comprehensive secondary stroke prevention protocols within a transition care program.
In light of the robust research supporting transition care and the critical need to enhance care quality and address preventable readmissions, several practical recommendations are essential for all patients under the care of neurohospitalists:
- Patient Engagement: Provide thorough counseling on medication management, educate patients and caregivers about “red flag” symptoms, disease-specific management strategies, and available resources to address post-discharge concerns.
- Communication with Outpatient Providers: Ensure seamless communication with outpatient providers, including rehabilitation facilities and skilled nursing facilities, to facilitate appropriate follow-up appointments, medication reconciliation, and ongoing care management.
- Outreach: Implement a system for post-discharge outreach, such as follow-up telephone calls or home visits when appropriate, to proactively ensure a safe and supported transition for every patient.
Footnotes
Authors’ Note: All statements expressed in this work are those of the authors and should not in any way be construed as official opinions or positions of the University of California, San Francisco, AHRQ, or the US Department of Health and Human Services.
Declaration of Conflicting Interests: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Stephanie Rennke is a consultant for the Society of Hospital Medicine’s Project BOOST.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by funding from the Agency for Healthcare Research and Quality (AHRQ), US Department of Health and Human Services (contract no. HHSA-290-2007-10062I).