
Hospitals are constantly seeking ways to refine their transitional care practices. The goal is clear: reduce the number of patients readmitted within 30 days, minimize adverse events, and ensure a smooth and safe transition for patients moving from the hospital environment back to their homes. Despite increased focus on transitional care, concrete reductions in readmission rates, especially for those with stroke and neurological conditions, remain elusive in many studies. The most promising Transitional Care Programs initiated by hospitals incorporate a “bridging” approach. This involves interventions both before and after discharge, guided by dedicated transitional care providers at multiple stages. While comprehensive strategies that prioritize patient involvement, dedicated transition teams, and streamlined communication with outpatient providers demand resources and time, evidence suggests that neurohospitalists can successfully implement transitional care programs. These programs are crucial for enhancing patient safety across the entire continuum of care.
 Figure 1.
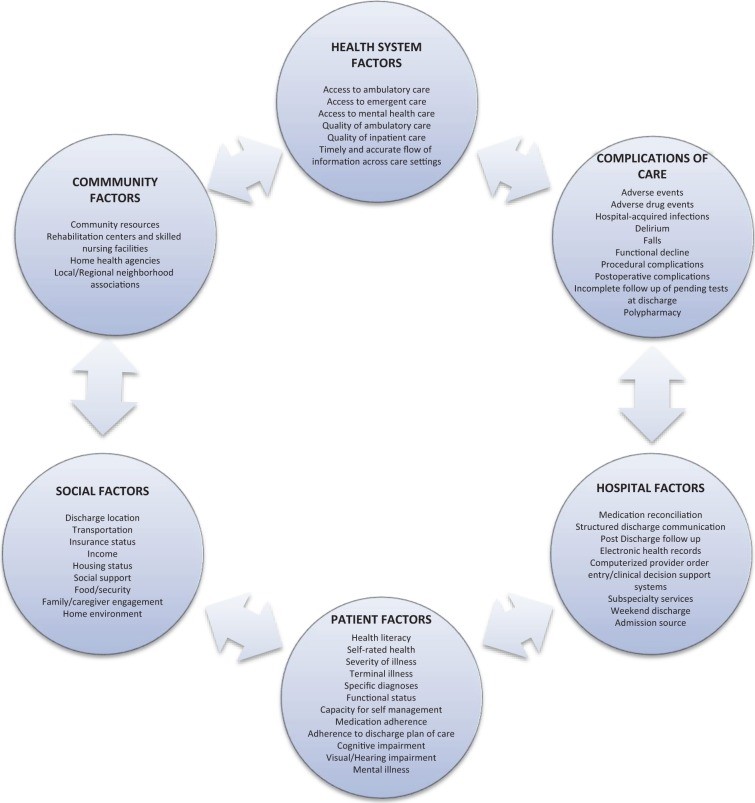
Figure 1.Factors Contributing to Hospital Readmission: Understanding the Web of Influences.
Introduction
The period immediately following a hospital stay is a vulnerable time for patients. Alarmingly, around one in five patients experience adverse events during this transition, including adverse drug events (ADEs) and complications arising from their hospital treatment. Readmission rates are also concerningly high, with nearly 20% of older Medicare patients returning to the hospital within 30 days of discharge.
A wide range of adverse events can occur post-discharge, spanning diagnostic and therapeutic errors. However, ADEs stand out as particularly prevalent and harmful, frequently leading to further hospitalizations and readmissions. Recent data indicates that approximately 100,000 elderly patients are hospitalized annually due to ADEs. Stroke patients are particularly vulnerable, facing elevated risks of recurrent cerebrovascular events, re-hospitalization within a year of their initial admission, increased disability, and higher mortality rates. For neurohospitalists, ensuring safe care transitions for neurologic patients—those with complex, chronic conditions like stroke, demyelinating diseases, epilepsy, and neuromuscular disorders—remains a critical patient safety priority.
Transitional care is defined as the care coordination patients receive as they navigate between different healthcare settings and providers. It aims to effectively bridge gaps in care across these transitions, such as from hospital to outpatient care. Hospital-based transitional care interventions are specifically designed to facilitate a smoother transition from inpatient to outpatient settings, thereby preventing avoidable readmissions and adverse events.
National policy initiatives are increasingly emphasizing improvements in transitional care, driven by the significant costs associated with adverse events and readmissions. The Centers for Medicare & Medicaid Services (CMS) already publicly reports hospitals’ risk-adjusted 30-day readmission rates for conditions like pneumonia, acute myocardial infarction, and congestive heart failure (CHF). It is expected that this reporting will expand to include other diagnoses, potentially encompassing neurological conditions such as stroke. CMS has already imposed financial penalties on over 2,000 hospitals due to high readmission rates, with penalties reaching up to 1% of Medicare reimbursements. The Partnership for Patients initiative set a goal to reduce preventable readmissions by 20% by the end of 2013, recognizing improved transitional care as a key strategy for lowering healthcare expenditures. These policies collectively mandate hospitals to prioritize and enhance transitional care for patients being discharged.
While highly focused, disease-specific transitional care programs have shown some success in reducing readmissions for conditions like CHF, chronic obstructive pulmonary disease, and asthma, effective strategies for neurological diseases are less clear. Numerous systematic reviews have examined a variety of interventions, but there is a lack of conclusive evidence regarding their impact on readmissions or other crucial indicators of post-discharge patient safety, such as emergency department (ED) visits and adverse events occurring after hospitalization.
Data suggests that nearly 20% of 30-day readmissions are potentially preventable. Hospital readmission rates are significantly influenced by factors outside the hospital’s direct control, including inadequate social support, poverty, and limited access to outpatient care. A recent review of stroke and cerebrovascular disease discharges from a single academic medical center revealed that 53% of readmissions were potentially avoidable. These avoidable readmissions were linked to issues such as gaps in care coordination, delayed follow-up appointments, and insufficient discharge instructions. Despite these ongoing challenges, progress is being made in readmission prevention, as evidenced by CMS reports indicating a decline in 30-day readmission rates for Medicare patients between 2007 and 2012.
In today’s healthcare landscape, where value-based care and cost-effectiveness are paramount, transitional care strategies are essential. Effective programs require a commitment of human resources, but they directly address core neurohospitalist and patient priorities: enhancing the quality of care delivered, prioritizing patient safety, and strengthening connections across healthcare systems. This review aims to describe key transitional care strategies, summarize the effectiveness of established programs, and provide actionable recommendations for neurohospitalists.
Transitional Care: Defining Strategies, Risks, and Key Approaches
Defining Transitional Care Strategies and Adverse Events
A “transitional care strategy” is defined as a specific intervention or a combination of interventions initiated before a patient is discharged from the hospital. The overarching goal is to ensure a safe and effective transition as patients move from one care setting to another, most commonly from the hospital back to their home. These interventions are broadly categorized into three types: predischarge interventions, postdischarge interventions, and “bridging” interventions, which incorporate elements of both pre- and postdischarge care.
Taxonomy of Interventions to Improve Transitional Care at Hospital Discharge
| Predischarge interventions | Postdischarge interventions | Bridging interventions |
|---|---|---|
| Risk assessment for adverse events or readmissions | Patient outreach (follow-up phone calls, hotlines, home visits) | Combination of at least one predischarge and one postdischarge component |
| Patient and caregiver education | Facilitated clinical follow-up (ambulatory provider follow-up) | |
| Creation of individualized patient records (lay language summaries) | Post-discharge medication reconciliation | |
| Facilitation of communication with outpatient providers | ||
| Multidisciplinary discharge planning teams | ||
| Dedicated transition providers (pre- and post-discharge contact) | ||
| Medication reconciliation |
Postdischarge adverse events are defined as clinically significant injuries or complications that occur after a patient leaves the hospital. These can include new or worsening symptoms, abnormal lab results requiring changes in treatment, and injuries such as ADEs, falls, or hospital-acquired infections that are at least partially attributable to hospital care. This definition aligns with classifications used in previous studies analyzing the occurrence of adverse events after discharge. Readmission itself is also considered an adverse event and is commonly measured at 30-day, 60-day, 90-day, and 6-month intervals following the initial hospitalization.
Identifying Readmission and Adverse Event Risks
Predicting precisely which patients will be readmitted or experience an adverse event remains challenging. However, certain patient groups are at higher risk during the post-hospitalization period. These include older adults, individuals with chronic illnesses, and those hospitalized for stroke. These populations are more susceptible due to potential gaps in healthcare quality, transitions across multiple care settings, and numerous handoffs between different providers. Factors such as poor functional status at discharge, advanced age, mental health conditions, and limited social support have been identified as risk factors for hospital readmission and poorer outcomes in neurology patients. Notably, a systematic review assessing predictors of readmission after stroke found a lack of standardized models for comparing or predicting readmissions across different hospitals.
Despite the absence of reliable prediction models, older adults and those with multiple chronic conditions constitute a significant portion of admissions and readmissions within inpatient neurology services. Stroke patients are frequently readmitted for cerebrovascular, cardiac, and non-cardiac issues, including urinary tract infections, pneumonia, and hip fractures.
Key Transitional Care Strategies: Effective Program Examples
Four transitional care strategies are particularly noteworthy due to evidence from controlled trials demonstrating their effectiveness in reducing readmissions.
Highlighted Hospital-Based Transitional Care Programs
| Program Name | Key Strategies | Description and Effectiveness |
|---|---|---|
| Care Transitions Intervention (CTI) | Patient engagement, individualized health record, dedicated transition provider, communication facilitation, outreach, medication reconciliation | Focuses on four core domains of self-management skills. Studied across various settings. Demonstrated significant reductions in 30-day readmission rates (ARR 3.6% – 5.8%) and 90-day readmission rates (ARR 5.8% – 21.7%). |
| Transitional Care Model (TCM) | Patient engagement, individualized health record, dedicated transition provider, communication facilitation, facilitated follow-up, outreach | Nurse-led program for geriatric patients, intensive home and telephone follow-up. Reduced 90-day readmission rates significantly (ARR 13% – 48%). |
| Project Re-Engineered Discharge (RED) | Patient engagement, individualized health record, dedicated transition provider, communication facilitation, multidisciplinary team, outreach, medication reconciliation (pre- and post-discharge) | Team-based approach with pharmacist involvement in outreach and medication reconciliation. Demonstrated reductions in combined ED visits and readmissions within 30 days. |
| Project Better Outcomes for Older Adults Through Safe Transitions (BOOST) | Patient engagement, multidisciplinary team, outreach, medication reconciliation, risk assessment | Quality improvement program implemented across multiple hospitals. Includes risk assessment, medication reconciliation, discharge checklists, and team-based approach. Showed modest reductions in 30-day readmission rates (ARR 2% – 5.9%). |
Abbreviations: ARR – Absolute Risk Reduction; ED – Emergency Department.
Care Transitions Intervention in Detail
The Care Transitions Intervention (CTI), developed by Eric Coleman at the University of Colorado, is a multi-faceted program implemented in numerous hospitals. Studies have included older adults admitted for stroke and other chronic illnesses. CTI’s primary goals are to empower patients and caregivers in self-management post-hospitalization and equip them with the skills to navigate the healthcare system effectively. The intervention is structured around four key pillars: (1) medication management, (2) personal health record development for seamless information transfer, (3) close follow-up with primary care providers, and (4) identification of “red flags” prompting patient-provider contact. A “transition coach,” typically an advanced practice nurse, conducts post-discharge home visits and phone calls, emphasizing patient engagement and self-management of chronic conditions. CTI has been rigorously studied in diverse acute care settings and has consistently shown statistically significant reductions in 30-day readmissions across managed care, capitated, and Medicare fee-for-service systems.
The Transitional Care Model in Detail
The Transitional Care Model (TCM), another nationally recognized program pioneered by Mary Naylor at the University of Pennsylvania, focuses on hospital-based discharge planning and home follow-up for high-risk, chronically ill older adults. It has also been studied in older adults with CHF and myocardial infarction, although specific inclusion of neurology patients in published studies is not noted. A transitional care nurse (TCN) guides patients through the transition from hospital to home, facilitates communication with outpatient providers, and conducts home visits and follow-up calls post-discharge. TCM emphasizes a multidisciplinary patient care approach, with the TCN acting as a central coordinator interacting with physicians, nurses, social workers, discharge planners, and pharmacists. Multiple studies have demonstrated significant reductions in readmission rates at both 60 and 90 days.
Project RED in Detail
Project Re-Engineered Discharge (RED) was studied in a general medicine population within an urban safety-net hospital. It emphasizes a multidisciplinary approach to patient care, coordinated by a nurse discharge advocate (DA). The DA engages patients during their hospital stay, providing clinical information and a personalized, illustrated post-hospitalization plan. Post-discharge, a pharmacist conducts telephone follow-ups, including medication reviews and direct communication with the patient’s primary outpatient provider. The initial Project RED study did not specify whether neurology patients were included. However, it demonstrated significant reductions in hospital utilization, defined as combined ED visits and readmissions, by approximately 30% within 30 days of discharge.
Project BOOST in Detail
Project Better Outcomes for Older Adults Through Safe Transitions (BOOST) is a transitional care program supported by the Society of Hospital Medicine. This quality improvement collaborative has been widely implemented across diverse US hospital settings, targeting general medicine and medical-surgical patient populations. Mentors, who are hospitalist experts in quality improvement and care transitions, guide hospitals in developing and implementing BOOST programs tailored to their specific needs. The BOOST toolkit includes interventions such as risk assessment, medication reconciliation, discharge checklists, and a multidisciplinary team approach to discharge processes. A study involving 30 hospitals showed modest reductions in readmission rates, although data was only available from 11 hospitals in the study.
Transitional Care Strategies for Neurologic Patients
Several studies have specifically evaluated the effectiveness of transitional care programs for stroke patients. A systematic review of 27 such studies concluded that limited evidence of low-to-moderate strength suggests hospital-initiated interventions can improve outcomes like reduced hospital stay duration and improved physical activity. However, these studies did not consistently demonstrate a reduction in readmissions or mortality. Despite the lack of clear evidence regarding healthcare utilization or adverse event reduction, study authors highlighted the importance of hospital-initiated strategies focused on care coordination for improving healthcare in this patient population. Specific interventions, such as secondary stroke prevention measures (antithrombotic, antihypertensive, and lipid-lowering medications), dysphagia screening, and reducing urinary catheter use in hospitals, have been shown to reduce readmissions and post-discharge adverse events like cerebrovascular accidents, pneumonia, and catheter-associated urinary tract infections. Neurohospitalists are uniquely positioned to positively impact patient care beyond the hospital stay by implementing interventions that improve care quality, reduce costs, and mitigate risks associated with preventable readmissions and adverse events.
Taxonomy of Interventions: A Framework for Enhancing Transitional Care at Hospital Discharge.
Common Elements of Effective Transitional Care Strategies
These successful transitional care programs share several common features. Both general programs and many stroke-specific programs incorporate bridging interventions, typically led by a dedicated transition provider, such as a nurse or case manager. A consistent emphasis is placed on having a patient advocate who facilitates care coordination and provides outreach to patients after they leave the hospital. Neurologic patients, similar to general medicine populations, benefit from strategies that prioritize improved communication across care settings, proactive patient outreach, and robust patient engagement.
Implementation and Cost Considerations
While descriptions of transitional care programs often detail timelines and interventions, information regarding costs, resource requirements for implementation, and sustainability strategies is often limited. Addressing these aspects is crucial for widespread adoption and long-term success of transitional care initiatives.
Discussion
This review has outlined a framework for understanding transitional care strategies aimed at decreasing hospital readmissions and post-discharge adverse events, highlighting four nationally recognized programs. A key finding is that nearly all effective transitional care programs published in the last two decades incorporate bridging interventions, typically relying on a dedicated transition provider who maintains contact with patients both before and after hospital discharge. Programs like CTI, Project BOOST, and TCM have been successfully implemented and evaluated across diverse patient populations and healthcare systems, with Project RED demonstrating success in a safety-net setting. While these strategies are resource-intensive, evidence supports their effectiveness. However, more information is needed regarding implementation processes, long-term sustainability, and detailed cost analyses. Further research is also necessary to fully understand the impact of these specific strategies on patients with acute neurological illnesses.
Recommendations for Neurohospitalists
Hospitals and neurohospitalists are challenged to determine the most effective transitional care services to offer patients post-hospitalization to minimize readmissions and avoid associated financial penalties. Current research points towards the success of multidisciplinary, multicomponent strategies utilizing bridging interventions and dedicated transition clinicians. Programs like CTI, TCM, Project RED, and Project BOOST have been studied and replicated across the US, providing valuable models. It’s important to recognize that each hospital network has unique internal factors, cultures, community demographics, and geographical considerations. A “one-size-fits-all” approach to transitional care is unlikely to be optimal. However, core elements of successful transitional care strategies include: patient engagement, dedicated transition providers, comprehensive medication management (including reconciliation), facilitated communication with outpatient providers, and proactive patient outreach. Neurology-specific interventions, such as home care protocols for disease monitoring, medication adherence support, symptom management guidelines, and direct connections with rehabilitation programs, can further enhance these strategies for neurologic patient populations.
Effective Transitional Care Programs: Key Strategies and Outcomes.
Summary Recommendations for Neurohospitalists
| Key Action Items for Implementing Transitional Care Programs |
|---|
| Analyze Hospital Readmission Data: Obtain 30-day readmission rates (overall and for specific units/diseases) to understand current performance and areas for improvement. |
| Assess Hospital Infrastructure: Evaluate existing quality improvement and patient safety infrastructure, including electronic health record capabilities and prior QI initiative experience. |
| Build an Interdisciplinary Team: Create a dedicated team with champions from different disciplines to drive and support transitional care program implementation. |
| Define Measurable Outcomes: Identify key metrics to track program success, such as 30-day readmission rates, adverse drug events, and medication errors. |
| Implement Multicomponent Strategies: Adopt a bundled approach that includes patient engagement, dedicated transition providers, medication reconciliation, communication facilitation, and patient outreach. |
| Incorporate Disease-Specific Interventions: Integrate neurology-specific interventions like secondary stroke prevention protocols and dysphagia screening into transitional care plans. |
Neurohospitalists, in their roles as both primary providers and consultants, are uniquely positioned to contribute expertise to enhance transitional care for a wide range of patients. For example, neurohospitalists can spearhead initiatives focused on delirium and dysphagia screening for patients with cerebrovascular and neurological diseases. They can also collaborate with general medicine hospitalists on broader, institution-wide transitional care strategies. As consultants, neurohospitalists can provide evidence-based recommendations to minimize readmission risks and other adverse events, such as implementing robust secondary stroke prevention measures.
Considering the evidence supporting transitional care and the critical need to improve care quality and address preventable readmissions, several practical recommendations are essential for all patients managed by neurohospitalists:
- Patient Engagement: Comprehensive counseling on medication management, recognition of warning signs (“red flags”), disease-specific management strategies, and available resources to address post-discharge concerns.
- Communication with Outpatient Providers: Ensure seamless communication with rehabilitation facilities and skilled nursing facilities, focusing on appropriate follow-up appointments, medication reconciliation, and ongoing care management.
- Proactive Patient Outreach: Implement follow-up telephone call services or home visits (when appropriate) to ensure a safe and supported transition for patients returning home.
Footnotes
Authors’ Note: The views expressed in this article are solely those of the authors and do not represent the official stances or opinions of the University of California, San Francisco, AHRQ, or the US Department of Health and Human Services.
Declaration of Conflicting Interests: Stephanie Rennke declares a potential conflict of interest as a consultant for the Society of Hospital Medicine’s Project BOOST.
Funding: This work was supported by funding from the Agency for Healthcare Research and Quality (AHRQ), US Department of Health and Human Services (contract no. HHSA-290-2007-10062I).